George Davey Smith challenges the findings of a new BMJ paper claiming that eating dark chocolate protects against Type 2 diabetes.
Xmas is supposed to be a time of goodwill, and medical journals like the BMJ print seasonal papers not intended to be taken too seriously. The topic of one of the latest papers – chocolate – has been the topic of Xmas BMJ papers in the past, but it appears this is intended to be a serious paper; it is certainly not entertaining. The paper suggests that dark chocolate can protect against type 2 diabetes. At the risk of being a Grinch at Christmas, it has to be said that this is, frankly, a meaningless paper. Indeed it is surprising to see such a paper published in 2024 in a supposedly reputable journal. (more…)
The idea that life’s little pleasures – a glass of red wine, for example – might be good for us is seductive. Given that most public health advice is simultaneously common sense and mildly dispiriting – eat healthily, exercise, don’t smoke – the possibility that we don’t have to live like Spartans to live long and healthily lives is surely good news… But is that really the case?
In this blog post, first published on the Institute of Alcohol Studies blog, Professor Marcus Munafò and Professor George Davey Smith of MRC Integrative Epidemiology Unit explain why confounding factors skew studies to suggest a small amount of alcohol might have health benefits, and how Mendelian randomization has debunked this common myth.(more…)
There’s a widespread belief that your testosterone can affect where you end up in life. At least for men, there is some evidence for this claim: several studies have linked higher testosterone to socioeconomic success. But a link is different to a cause and using DNA, our new research suggests it may be much less important for life chances than previously claimed.
In previous studies, male executives with higher testosterone have been found to have more subordinates, and financial traders with higher testosterone found to generate greater daily profits. Testosterone has been found to be higher among more highly educated men, and among self-employed men, suggesting a link with entrepreneurship. Much less is known about these relationships in women, but one study suggested that for women, disadvantaged socioeconomic position in childhood was linked to higher testosterone later in life.
The beneficial influence of testosterone is thought to work by affecting behaviour: experiments suggest that testosterone can make a person more aggressive and more risk tolerant, and these traits can be rewarded in the labour market, for instance in wage negotiations. But none of these studies show definitively that testosterone influences these outcomes because there are other plausible explanations.
Rather than testosterone influencing a person’s socioeconomic position, it could be that having a more advantaged socioeconomic position raises your testosterone. In both cases, we would see a link between testosterone and social factors such as income, education and social class.
There are plausible mechanisms for this too. First, we know that socioeconomic disadvantage is stressful, and chronic stress can lower testosterone. Second, how a person perceives their status relative to others in society might influence their testosterone: studies of sports matches, usually between men, have often found that testosterone rises in the winner compared to the loser.
Chronic stress can lower your testosterone. Shutterstock
It’s also possible that some third factor is responsible for the associations seen in previous studies. For instance, higher testosterone in men is linked to good health – and good health may also help people succeed in their careers. A link in men between testosterone and socioeconomic position could therefore simply reflect an impact of health on both. (For women, higher testosterone is linked to worse health, so we would expect an association of higher testosterone and lower socioeconomic position.)
Look at it this way
It is very difficult to pick apart these processes and study just the effects of testosterone on other things. With this goal in mind, we applied a causal inference approach called “Mendelian randomisation”. This uses genetic information relevant to a single factor (here, testosterone) to isolate just the effect of that factor on one or more outcomes of interest (here, socioeconomic outcomes such as income and educational qualifications).
DNA can tell us a lot about our relationship with testosterone. Zita/Shutterstock
A person’s circulating testosterone can be affected by environmental factors. Some, like the time of day, are straightforward to correct for. Others, like somebody’s health, are not. Crucially, socioeconomic circumstances could influence circulating testosterone. For this reason, even if we see an association between circulating testosterone and socioeconomic position, we cannot determine what is causing what.
This is why genetic information is powerful: your DNA is determined before birth and generally does not change during your lifetime (there are rare exceptions, such as changes which occur with cancer). Therefore, if we observe an association of socioeconomic position with genetic variants linked to testosterone, it strongly suggests that testosterone is causing the differences in socioeconomic outcomes. This is because influence on the variants of other factors is much less likely.
In more than 300,000 adult participants of the UK Biobank, we identified genetic variants linked to higher testosterone levels, separately for men and women. We then explored how these variants were related to socioeconomic outcomes, including income, educational qualifications, employment status, and area-level deprivation, as well as self-reported risk-taking and overall health.
Similar to previous studies, we found that men with higher testosterone had higher household income, lived in less deprived areas, and were more likely to have a university degree and a skilled job. In women, higher testosterone was linked to lower socioeconomic position, including lower household income, living in a more deprived area, and lower chance of having a university degree. Consistent with previous evidence, higher testosterone was associated with better health for men and poorer health for women, and more risk-taking for men.
However, there was little evidence that genetic variation related to testosterone affected socioeconomic position at all. In both men and women we detected no effects of genetic variants related to testosterone on any aspect of socioeconomic position, or health, or risk-taking.
Because we identified fewer testosterone-linked genetic variants in women, our estimates for women were less precise than for men. Consequently, we could not rule out relatively small effects of testosterone on socioeconomic position for women. Future studies could examine associations in women using larger, female-specific samples.
But for men, our genetic results clearly suggest that previous studies may have been biased by the influence of additional factors, potentially including the impact of socioeconomic position on testosterone. And our results indicate that – despite the social mythology surrounding testosterone – it may be much less important for success and life chances than earlier studies have suggested.
‘Enhancing the utilization of COVID-19 testing in schools’, is a study which will look at the characteristics of long COVID and COVID-19 infection in children. ‘Long COVID’ is commonly used to describe signs and symptoms that continue or develop after acute COVID‑19. The study is being funded as a result of a rapid funding call by Health Data Research UK (HDR UK), the Office for National Statistics (ONS) and UK Research and Innovation (UKRI). The study forms part of the larger Data and Connectivity National Core Study, which is led by HDR UK in partnership with ONS.
The COVID-19 testing in schools study is related to the CoMMinS (COVID-19 Mapping and Mitigation in Schools) study being undertaken by the University of Bristol in partnership with Bristol City Council, Public Health England [PHE] and Bristol schools. CoMMinS aims to give us an understanding of COVID-19 infection dynamics centred around school pupils and staff and onward transmission to family contacts, using regular testing. Our study will jointly analyse data from CoMMinS, along with information from Electronic Patient Records, and data from the COVID-19 Schools Infection Survey (SIS; jointly led by the London School of Hygiene & Tropical Medicine [LSHTM], PHE, and ONS). The SIS is a study similar to CoMMinS but carried out nationally.
To help inform research questions and methods for the study, members from the University of Bristol study team gathered views about long COVID in children between 9 March and 30 April 2021 from:
seven young people from the NIHR Bristol Biomedical Research Centre Young People’s Advisory Group (YPAG)
five families whose children have long COVID or suspected long COVID, recruited through two online UK campaign groups for long COVID, and
a survey completed by four GPs and one paediatrician, and an online meeting with two paediatricians.
It is important to note that the opinions gathered were based on small samples which may not be representative.
Through the meeting and survey with the doctors, the study team found that clinical understanding of long COVID in children is currently very limited.
The doctors said that it may be hard to distinguish between long COVID and other conditions with similar symptoms. Many of the symptoms of long COVID, like fatigue and feeling sick, aren’t very specific, and are common to many different conditions. Long COVID in children currently lacks a clinical definition, making diagnosis difficult. It isn’t yet properly understood whether long COVID is a new condition in itself, or a group of conditions like post viral fatigue, which is already recognised.
Young people, and families of children with long COVID or suspected long COVID, who were also asked for their opinion, said that feeling sick or stomach pain, extreme tiredness, and headaches were the symptoms they would rank as most ‘harmful’. For young people, this was based on them imagining having the symptoms. For the families, this was based on their first-hand experience.
The families also said that the symptoms their children were experiencing were numerous, often very severe, and more wide-ranging than those currently listed on the NHS website for long COVID. It is not yet clear what is causing the unusual symptoms.
The families said that they had struggled to get a diagnosis and treatment for their children. They also said that long COVID symptoms were having a significant impact on their children’s day-to-day lives both physically and psychologically, and that some of the children had missed school because of the symptoms. Some of the families also found fevers difficult to manage because their children had to miss school to self-isolate every time they had a fever. They wanted to know why the set of symptoms were being experienced, and why their children in particular had developed them.
It is not known how many children have or will develop long COVID. So far, studies which have tried to measure the rate of long COVID in children suggest it is rare. However, quantifying the number of cases is made difficult by a lack of clinical understanding of long COVID including the lack of an agreed clinical definition. The opinions collected suggest that relying on clinical diagnoses alone will under-estimate cases. On the other hand, there needs to be a cautious approach to estimating the number of cases based on non-specific symptoms, as other conditions which cause similar symptoms may be counted as well.
Caroline Relton, Professor of Epigenetic Epidemiology and Director of the Bristol Population Health Science Institute at the University of Bristol, joint lead for CoMMinS and one of the lead authors of the report, said: “The opinions we gathered further highlight that it is difficult to count the number of children with long COVID on the basis of diagnoses alone while long COVID in children remains poorly defined.
“There are added complications of studying long COVID in children, when it is sometimes difficult to disentangle what might be the result of experiencing infection from what might result from the wider impact of experiencing the pandemic. Isolation, school closures, disrupted education and other influences on family life could all have health consequences. Defining the extent of the problem in children and the root causes will be essential to helping provide the right treatment and to aid the recovery of young people who are suffering.”
The findings highlight that examining GP and hospital visits, and school attendance, might currently be a more useful and feasible way of assessing how COVID-19 has affected children, rather than relying only on diagnoses of long COVID. However, the study researchers also need to be aware how often healthcare is accessed according to need, and absence from school due to self-isolation, which will affect what is being measured.
Feeling sick or stomach pain, extreme tiredness, and headaches will be important symptoms to consider in the study.
Leaving the EU presents many unique challenges to Britain, among which is the crucial task of maintaining ourhigh levels of food safety. As a submission to the Jean Golding Institute’s data visualisation competition,we briefly investigated the impacts that Brexit mayhave on British food supplies.The dataset used in this analysis was made available by the Food Standards Agency (FSA)as the focus of the competition, and all code used is freely available in ourgithub repository.
The Need for Information Recompense
In the first part of the analysis, we exploredcases where food imported to Britainled toan alert being raised. The two biggest sources for such alerts were Britain’s internal alert systems (largely the FSA), and the EU’s Rapid Alert System for Food and Feed (RASFF).
Since Britain is on course tolose access to RASFF-supplied information once Brexit is finalised in early 2021, we created the visualisation below as a comparisonof the FSA and the RASFF in terms of both the numberof alerts raisedand the corresponding food’s origin country for each alert.
Alerts from the EU Alert System
The arcs show the countries of origin ofimports that raised alerts, and the yellow-red density map shows the recordedhazard alert frequency from those origins.Interactive versions ofthe two map instancescan be foundby following these links: RASFF, UK internal alerts.
Alerts from the UK Alert System
If the UK does indeed loseaccess to the RASFF, the loss of food hazards information about our own imports will be tremendous. The burden then falls on the FSA to develop and extend their alert system (which currently focuses very little on internationally supplied food) to bridge this information gap and ensure food safety forgloballyimported goods.As of the time of writing weare unsure what steps are being taken by the FSA, or the government at large, to address this issue.
Post-Brexit Shifts in Food Hazard Threats
As an extension of this work, we turned our attention to tariffs and the effect they might have on whom Britain chooses to import from. Upon leaving the EU the UK will have to negotiate new trade deals with both EU and non-EU countries.Sincethe cost forEU-produced food is expected to rise for Britain after Brexit, wemayindeed see Britain importing more from outside of the union, which would naturally bring a shift to the make–up of food hazards that our alert systems will need to detect. Anticipating this shift will allow us to better mitigate the accompanying risk if it does begin to materialise.
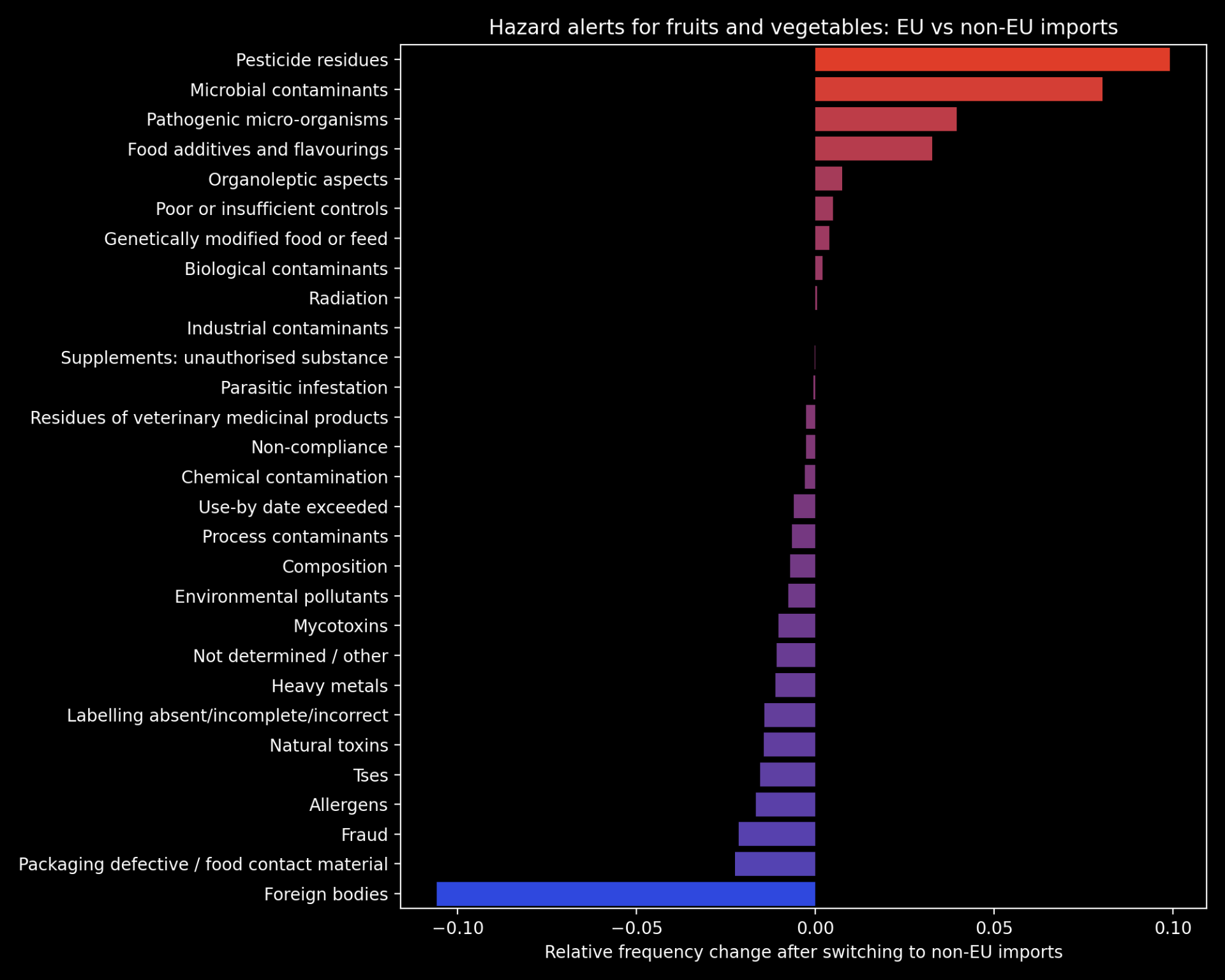
To this end, we explored the differences in food hazard threats posed by EU vs non-EU suppliers of Britain’s largest class of imported food: fruits and vegetables. The plot below shows the relative change in frequency for each category of food hazard in the case that Britain switched from 100% EU imports of fruit and vegetables to 100% non-EU. The hazard categories that are likely to increase in non-EU imports are highlighted in red. Please note that this is the most extreme case possible and is unlikely to unfold to this extent inreality– this plot is therefore presented as aguide to the different food threats posed by EU vs non-EU imports.
Hazard alerts for fruits and vegetables: EU vs non-EU imports
Our full submission‘Too Much Tooty in the Fruity: Keeping Food Safe in a Post-Brexit Britain’ can be found here, and includes a further breakdown of some of the categories of hazards displayed in the chart above. This work was awarded one of two joint runner-up prizes of the competition, tied with Angharad Stell’sShiny app:‘From a data space to knowledge discovery’. The winner of the competition was Robert Eyre, who producedthis impressive visualization dashboard using D3.The Jean Golding Institute are hosting a showcase event on the 18th November, where all competition entries will be presented.
We would like to thank theJGI for hosting the competition, and our PhD supervisors, Prof. Tom Gaunt and Dr. Ben Elsworth, for encouraging us to enter.
 Xmas is supposed to be a time of goodwill, and medical journals like the BMJ print seasonal papers not intended to be taken too seriously. The topic of one of the latest papers – chocolate – has been the topic of Xmas BMJ papers in the past, but it appears this is intended to be a serious paper; it is certainly not entertaining. The paper suggests that dark chocolate can protect against type 2 diabetes. At the risk of being a Grinch at Christmas, it has to be said that this is, frankly, a meaningless paper. Indeed it is surprising to see such a paper published in 2024 in a supposedly reputable journal. (more…)
Xmas is supposed to be a time of goodwill, and medical journals like the BMJ print seasonal papers not intended to be taken too seriously. The topic of one of the latest papers – chocolate – has been the topic of Xmas BMJ papers in the past, but it appears this is intended to be a serious paper; it is certainly not entertaining. The paper suggests that dark chocolate can protect against type 2 diabetes. At the risk of being a Grinch at Christmas, it has to be said that this is, frankly, a meaningless paper. Indeed it is surprising to see such a paper published in 2024 in a supposedly reputable journal. (more…)