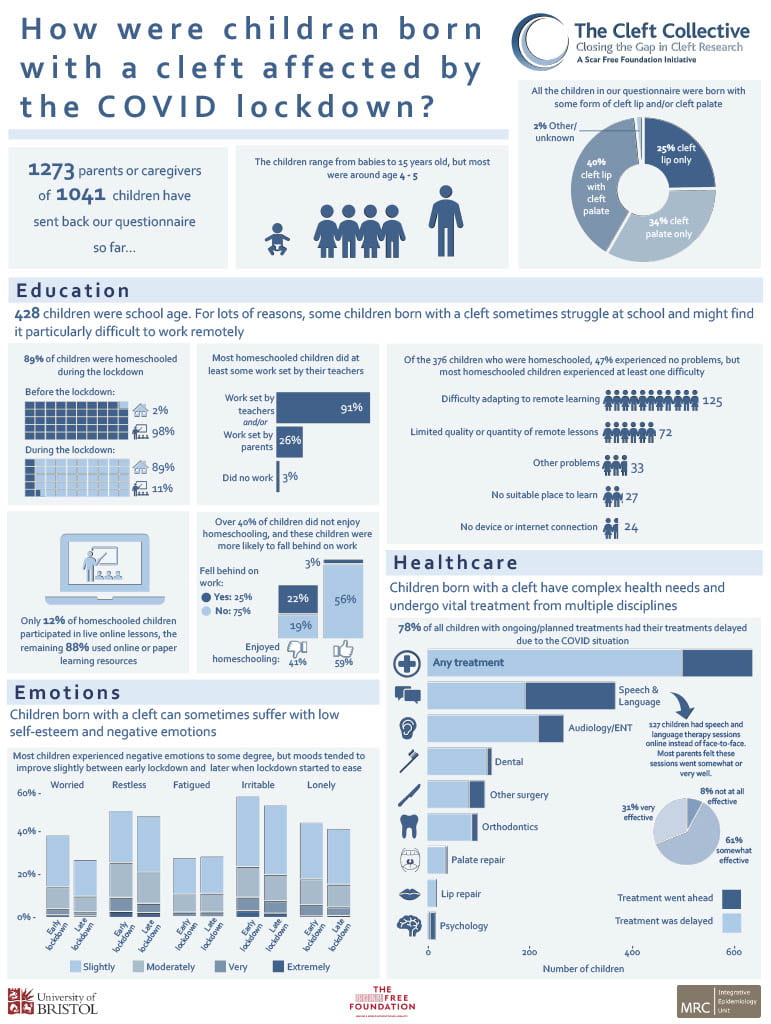
The COVID-19 pandemic has been difficult for many families and there is widespread concern about how the lockdown might have affected children’s health, wellbeing and education. This concern may be even greater for families of children with pediatric health conditions such as cleft lip and/or cleft palate.
The Cleft Collective cohort study, linked to the IEU, is a UK-wide research study of the causes and consequences of being born with a cleft, which is a gap in the lip or roof of the mouth. In response to the COVID-19 lockdown, the Cleft Collective team sent out a questionnaire asking parents about how the lockdown had affected their children’s surgeries and treatments, access to schooling and wellbeing.
The first results are summarised in this infographic, which highlights that many children suffered delays in their surgeries and other health care appointments due to the lockdown. They also struggled with homeschooling, worries and negative emotions.
Through links to the NHS cleft teams and the Cleft Lip and Palate Association charity (CLAPA), the Cleft Collective team are sharing their findings with healthcare professionals to help ensure that children born with a cleft are given appropriate support to help them through this time and to lead happy, healthy childhoods.
The Cleft Collective cohort study is based in the MRC Integrative Epidemiology Unit and funded by the Scar Free Foundation and the University of Bristol. The video below explains more about the study.
Gareth J Griffith, Gibran Hemani, Annie Herbert, Giulia Mancano, Tim Morris, Lindsey Pike, Gemma C Sharp, Matt Tudball, Kate Tilling and Jonathan A C Sterne, together with the authors of a preprint on collider bias in COVID-19 studies.
All authors are members of the MRC Integrative Epidemiology Unit at the University of Bristol. Jonathan Sterne is Director of Health Data Research UK South West
Among successful actors, being physically attractive is inversely related to being a good actor. Among American college students, being academically gifted is inversely related to being good at sport.
Among people who have had a heart attack, smokers have better subsequent health than non-smokers. And among low birthweight infants, those whose mothers smoked during pregnancy are less likely to die than those whose mothers did not smoke.
These relationships are not likely to reflect cause and effect in the general population: smoking during pregnancy does not improve the health of low birthweight infants. Instead, they arise from a phenomenon called ‘selection bias’, or ‘collider bias’.
Understanding selection bias
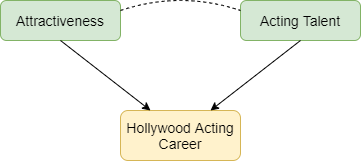
Selection bias occurs when two characteristics influence whether a person is included in a group for which we analyse data. Suppose that two characteristics (for example, physical attractiveness and acting talent) are unrelated in the population but that each causes selection into the group (for example, people who have a successful Hollywood acting career). Among individuals with a successful acting career we will usually find that physical attractiveness will be negatively associated with acting talent: individuals who are more physically attractive will be less talented actors (Figure 1). Selection bias arises if we try to infer a cause-effect relationship between these two characteristics in the selected group. The term ‘collider bias’ refers to the two arrows indicating cause and effect that ‘collide’ at the effect (being a successful actor).
Figure 1: Selection effects exerted on successful Hollywood actors. Green boxes highlight characteristics that influence selection. Yellow boxes indicate the variable selected upon. Arrows indicate causal relationships: the dotted line indicates a non-causal induced relationship that arises because of selection bias.
Figure 2 below explains this phenomenon. Each point represents a hypothetical person, with their level of physical attractiveness plotted against their level of acting talent. In the general population (all data points) an individual’s attractiveness tells us nothing about their acting ability – the two characteristics are unrelated. The red data points represent successful Hollywood actors, who tend to be more physically attractive and to be more talented actors. The blue data points represent other people in the population. Among successful actors the two characteristics are strongly negatively associated (green line), solely because of the selection process. The direction of the bias (whether it is towards a positive or negative association) depends on the direction of the selection processes. If they act in the same direction (both positive or both negative) the bias will usually be towards a negative association. If they act in opposite directions the bias will usually be towards a positive association.
Figure 2: The effect of sample selection on the relationship between attractiveness and acting talent. The green line depicts the negative association seen in successful actors.
Why is selection bias important for COVID-19 research?
In health research, selection processes may be less well understood, and we are often unable to observe the unselected group. For example, many studies of COVID-19 have been restricted to hospitalised patients, because it was not possible to identify all symptomatic patients, and testing was not widely available in the early phase of the pandemic. Selection bias can seriously distort relationships of risk factors for hospitalisation with COVID-19 outcomes such as requiring invasive ventilation, or mortality.
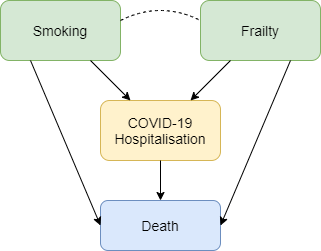
Figure 3 shows how selection bias can distort risk factor associations in hospitalised patients. We want to know the causal effect of smoking on risk of death due to COVID-19, and the data available to us is on patients hospitalised with COVID-19. Associations between all pairs of factors that influence hospitalisation will be distorted in hospitalised patients. For example, if smoking and frailty each make an individual more likely to be hospitalised with COVID-19 (either because they influence infection with SARS-CoV-2 or because they influence COVID-19 disease severity), then their association in hospitalised patients will usually be more negative than in the whole population. Unless we control for all causes of hospitalisation, our estimate of the effect of any individual risk factor on COVID-19 mortality will be biased. For example, it would be unsurprising that within hospitalised patients with COVID-19 we observe that smokers have better health than non-smokers because they are likely to be younger and less frail, and therefore less likely to die after hospitalisation. But that finding may not reflect a protective effect of smoking on COVID-19 mortality in the whole population.
Figure 3: Selection effects on hospitalisation with COVID-19. Box colours are as in Figure 1. Blue boxes represent outcomes. Arrows indicate causal relationships, the dotted line indicates a non-causal induced relationship that arises because of selection bias.
Selection bias may also be a problem in studies based on data from participants who volunteer to download and use COVID-19 symptom reporting apps. People with COVID-19 symptoms are more likely to use the app, and so are people with other characteristics (younger people, people who own a smartphone, and those to whom the app is promoted on social media). Risk factor associations within app users may therefore not generalise to the wider population.
What can be done?
Findings from COVID-19 studies conducted in selected groups should be interpreted with great caution unless selection bias has been explicitly addressed. Two ways to do so are readily available. The preferred approach uses representative data collection for the whole population to weight the sample and adjust for the selection bias. In absence of data on the whole population, researchers should conduct sensitivity analyses that adjust their findings based on a range of assumptions about the selection effects. A series of resources providing further reading, and tools allowing researchers to investigate plausible selection effects are provided below.
Dahabreh IJ and Kent DM. Index Event Bias as an Explanation for the Paradoxes of Recurrence Risk Research. JAMA 2011; 305(8): 822-823.
Griffith, Gareth, Tim M. Morris, Matt Tudball, Annie Herbert, Giulia Mancano, Lindsey Pike, Gemma C. Sharp, Jonathan Sterne, Tom M. Palmer, George Davey Smith, Kate Tilling, Luisa Zuccolo, Neil M. Davies, and Gibran Hemani. Collider Bias undermines our understanding of COVID-19 disease risk and severity.Interactive App 2020 http://apps.mrcieu.ac.uk/ascrtain/
Back in May, IEU researcher Dr Gemma Sharp took part in Creative Reactions, an initiative that pairs scientists with artists to create artwork based on their academic research. With 50 artists and 50 scientists collaborating on works from sculptures and wood carvings to canvas, digital and performance art, the 2019 exhibition ran across two venues in Bristol.
Gemma was paired with Olga Trevisan, an artist based in Venice, Italy. They had conversations over Skype where they spoke about their work and formed some initial ideas about how they could combine their interests in a new way while remaining coherent to their own practices. Reflecting on the collaboration, Olga said, “I love how curious you can be of a subject you haven’t considered before. I believe collaboration helps to open your own mind.”
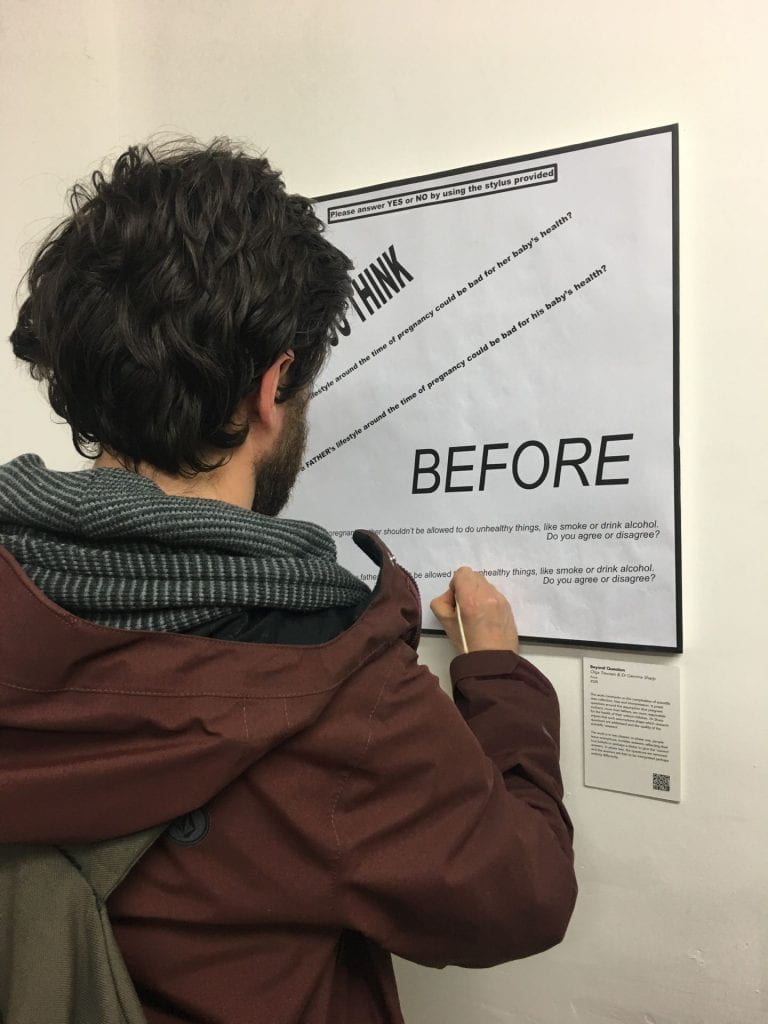
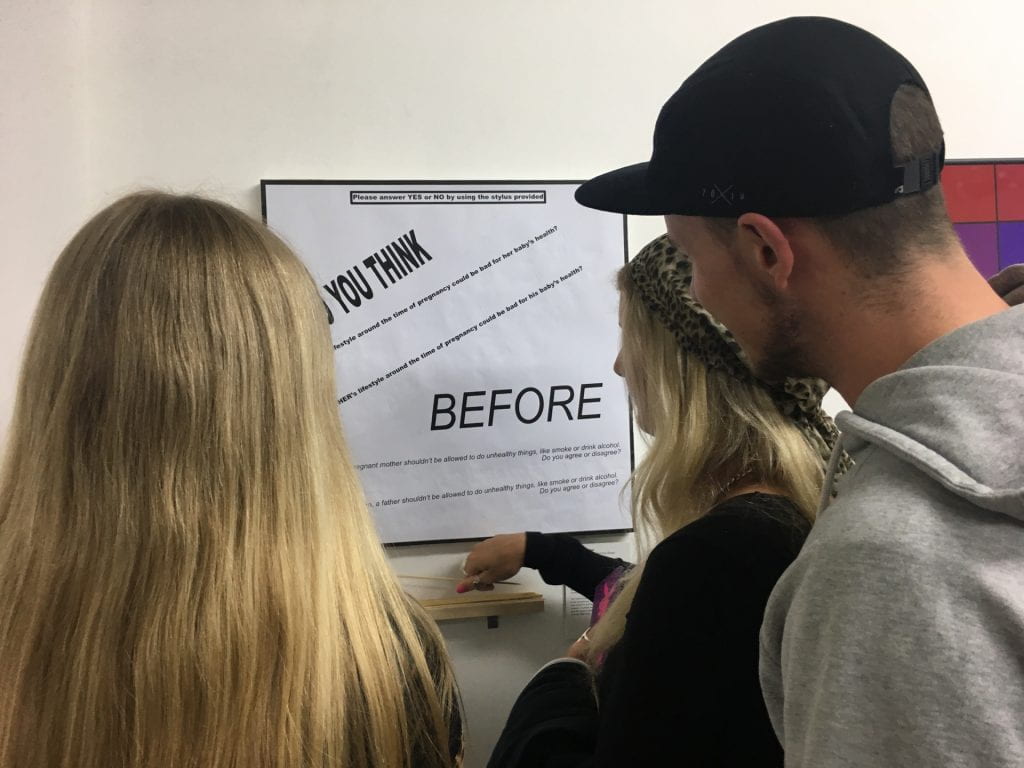
Based on some of the work around EPoCH, Olga created a piece called Beyond Question, which comments on the complexities of scientific data collection, bias and interpretation.
It poses questions around the pervasive assumption that pregnant women are more responsible for the (ill) health of their unborn children than their male partners are. Gemma and colleagues have argued that such assumptions drive the research agenda and the public perception of parental roles, by shaping which research questions get asked, which data are collected, and the quality of the scientific ‘answer’.
Photo credit: Olga Trevisan
Beyond Question was presented in two phases at two separate exhibitions: during the first phase, people were invited to answer questions with a simple Yes or No using a stylus; leaving no marks but only invisible, anonymous traces on the surface below. Answers will reflect the real assumptions, beliefs and attitudes of the respondent, but perhaps also, despite anonymity, their eagerness to ‘please’ the questioners, to give the ‘right’ answer, and to mask their true responses to paint themselves in the ‘best’ light.
In the second phase, the questions were removed and the answer traces were left alone to carry their own meaning; free to be combined with the attitudes, beliefs and assumptions of the viewer and to be interpreted and judged in perhaps an entirely different way.
Photo credit: Olga Trevisan
The questions posed were:
“Do you think a mother’s lifestyle around the time of pregnancy could be bad for her baby’s health?”
“Do you think a father’s lifestyle around the time of pregnancy could be bad for his baby’s health?”
“Before her baby is born, a pregnant mother shouldn’t be allowed to do unhealthy things, like smoke or drink alcohol. Do you agree or disagree?”
“Before his baby is born, a father shouldn’t be allowed to do unhealthy things, like smoke or drink alcohol. Do you agree or disagree?”
A novel thing about the Exploring Prenatal influences On Childhood Health (EPoCH) study is that we’re not just focusing on maternal influences on offspring health, we’re looking at paternal influences as well.
One of the reasons that most other studies have focused on maternal factors is that it’s perhaps easier to see how mothers might have an effect on their child’s health. After all, the fetus develops inside the mother’s body for nine months and often continues to be supported by her breastmilk throughout infancy. However, in a new paper from me and Debbie Lawlor published in the journal Diabetologia, we explain that there are lots of ways that fathers might affect their child’s health as well, and appreciating this could have really important implications. The paper focuses on obesity and type two diabetes, but the points we make are relevant to other health traits and diseases as well.
The EPOCH study will look at how much paternal factors actually causally affect children’s health. Image by StockSnap from Pixabay
How could fathers influence the health of their children?
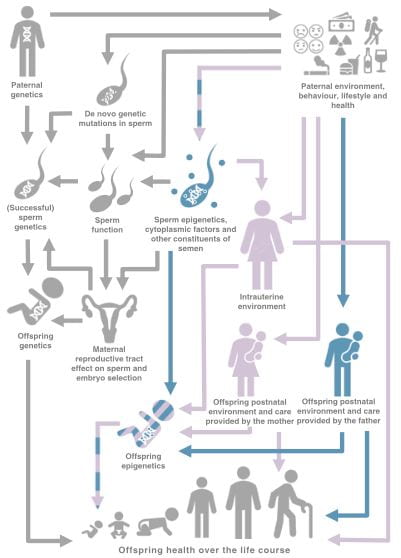
These are the main mechanisms we discuss in the paper:
Through paternal DNA. A father contributes around half of their child’s DNA, so it’s easy to see how a father’s genetic risk of disease can be transmitted across generations. Furthermore, a father’s environment and behaviour (e.g. smoking) could damage sperm and cause genetic mutations in sperm DNA, which could be passed on to his child.
Through “epigenetic” effects in sperm. The term “epigenetics” refers to molecular changes that affect how the body interprets DNA, without any changes occurring to the DNA sequence itself. Some evidence suggests that a father’s environment and lifestyle can cause epigenetic changes in his sperm, that could then be passed on to his child. These epigenetic changes might influence the child’s health and risk of disease.
Through a paternal influence on the child after birth. There are lots of ways a father can influence their child’s environment, which can in turn affect the child’s health. This includes things like how often the father looks after the child, his parenting style, his activity levels, what he feeds the child, etc.
Through a father’s influence on the child’s mother. During pregnancy, a father can influence a mother’s environment and physiology through things like causing her stress or giving her emotional support. This might have an effect on the fetus developing in her womb. After the birth of the child, a father might influence the type and level of child care a mother is able to provide, which could have a knock-on effect on child health.
There are lots of ways in which fathers might influence the health of their offspring. This figure was originally published in our paper in Diabetologia (rdcu.be/bPCBa).
What does this mean for public health, clinical practice and society?
Appreciating the role of fathers means that fathers could be given advice and support to help improve offspring health, and their own. Currently hardly any advice is offered to fathers-to-be, so this would be an important step forward. Understanding the role of fathers would also help challenge assumptions that mothers are the most important causal factor shaping their children’s health. This could help lessen the blame sometimes placed on mothers for the ill health of the next generation.
What’s the current evidence like?
In the paper, we reviewed all the current literature we could find on paternal effects on offspring risk of obesity and type 2 diabetes. We found that, although there have been about 116 studies, this is far less than the number of studies looking at maternal effects. Also, a lot of these studies just show correlations between paternal factors and offspring health (and correlation does not equal causation!).
What is needed now is a concerted effort to find out how much paternal factors actually causally affect offspring health. This is exactly what EPoCH is trying to do, so watch this space!
This content was reposted with permission from the EPOCH blog.
For many years, researchers have been studying how our early life experiences, including those that happen before we are born, can affect our lifelong health. In an article we wrote last year, Debbie Lawlor (University of Bristol), Sarah Richardson (Harvard University) and I show that most of these studies have focused on the characteristics and behaviours of mothers around the time of pregnancy. In a recent paper published in the Journal of Developmental Origins of Health and Disease, Debbie Lawlor, Sarah Richardson, Laura Schellhas and I show that there have been more studies of maternal prenatal influences on offspring health than any other factors (read more here).
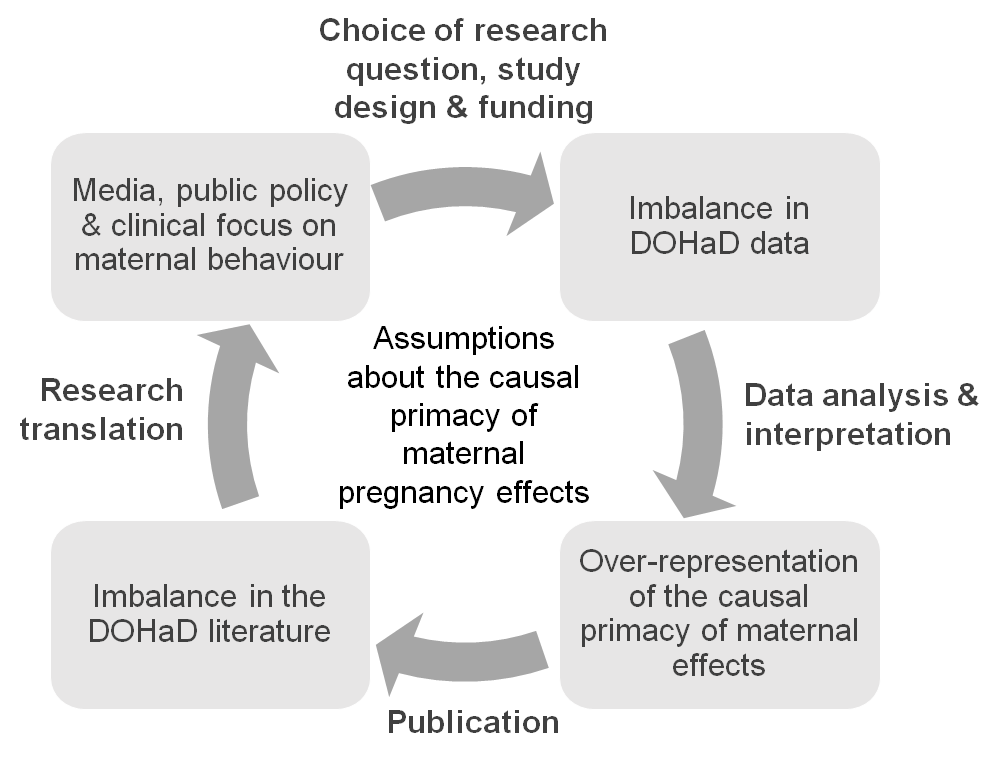
We argue this is because people assume that mothers, through their connection to the developing fetus in the womb, are the single most important factor in shaping a child’s health. This assumption runs deep and is reinforced at every level, from researchers, to research funders, to journalists, to policy makers, to health care professionals and the general public (see figure 1).
In our article, we question the truth behind this assumption.
Is there a strong scientific rationale for studying pregnant mothers so intensively?
Well, no actually. Although a lot of studies have found correlations between maternal characteristics and offspring health, the evidence that these characteristics actually have a causal effect is pretty weak. And since there haven’t been many studies of the effects of fathers and other factors, it’s difficult to say how important any maternal effect might be compared to any other early life experience.
Focusing so intensively on pregnant mothers, and interpreting all evidence as causal (if a mother does X, their unborn child will have Y), can have very damaging effects. Complex, nuanced scientific findings are being rushed into simplified advice that, although well-meaning, places the burden of blame on individual pregnant women. For example, there has been very little research on the effects of low-level drinking during pregnancy, but the current advice in the United States is for all sexually active women of reproductive age to avoid alcohol completely if they are not using birth control, for fear of fetal harm.
Fig. 1 Assumptions that the health, lifestyle and behaviours of mothers around the time of pregnancy have the largest causal influence on their children’s health and risk of disease drives research at all stages, from study design to research translation, and is also reinforced by research itself.
A culture of blame
The culture of blame is more overt in the media, where articles are often guilty of scaremongering. This feeds into public beliefs about how pregnant women should and shouldn’t behave, which can limit pregnant women’s freedom and even lead to questions around whether their behaviour is criminal. For example, pregnant women have reportedly been refused alcoholic drinks in bars, and taking drugs during pregnancy is legally classed as child abuse in many US states.
In our article, we make a number of recommendations that we hope will create more of a balance. In particular, we call for more research on how child health might be influenced by fathers and other factors, including the social conditions and inequalities that influence health behaviours. We also call for greater attention to be paid to how health advice to pregnant women is constructed and conveyed, with clear communication of the supporting scientific evidence to allow individuals to form their own opinions.
The EPoCH study
In June, I’ll begin work on a new project to investigate how both mothers and fathers’ lifestyles might causally affect the health of their children. Funded by the Medical Research Council, the EPoCH (Exploring Prenatal influences on Childhood Health) study will highlight whether attempts to improve child health are best targeted at mothers, fathers or both parents. I’m excited to work closely with the people behind WRISK to help ensure that findings from this project are communicated effectively and responsibly.
I hope that, along with the rest of the research community, we can produce high quality evidence to support health care and advice that maximises the health of all family members and stops blaming women for the ill health of the next generation.
The original article can be accessed (open access) here, and the authors’ full list of recommendations can be found below.
Full recommendations
Our full recommendations, which apply variously to researchers, journalists, policy makers and clinicians:
Collect more and better quality data on partners of pregnant women.
In addition to studying the effects of mothers, study and compare the effects of partners/fathers, social and other factors on child health.
Look for causal relationships between these factors and child health, not just (potentially spurious) correlations.
Publish all results, including negative results, to give a balanced view of the evidence.
Be aware and critical of the current imbalance in the scientific literature and how this will bias our overall understanding of the truth.
Collaborate with social scientists to consider the social implications of this research and the role of cognitive bias and social assumptions when interpreting findings.
When communicating findings, put the risk in context: compare findings to the broader scientific literature and the social environment.
Avoid language that suggests individual mothers are responsible for direct harm to their foetuses (most of the evidence will be based on averages in a population and can’t be assumed to apply to all individuals).
Where there is evidence of a paternal effect, aim public health advice at both parents.
Explain the level of risk in a way that empowers people to assess the evidence and form their own opinions (i.e. avoid over simplification).
This blog post is an edited version of one originally posted on the WRISK project website.