Inflammation is thought to play a role in depression. According to research that combined information from many studies (i.e., systematic review and meta-analysis), approximately a quarter of all those diagnosed with depression also have consistently higher levels of inflammatory proteins, like C-reactive protein (CRP), in their blood. Large population-based studies and studies using genetic information (i.e., Mendelian Randomization) further suggest that inflammation, particularly an inflammatory protein called interleukin 6 (IL-6), play a key role in causing depression. (You can read more about the role of inflammation in depression in our IEUREKA blog on “Immune cells as biomarkers of depression”.)
So far, studies examining this relationship between inflammation and depression have only focused on the levels of individual immune proteins in the blood, like IL-6 and CRP. At a cellular level, an inflammatory response is not caused by the activity of one inflammatory protein but rather by the interaction between several proteins working together to trigger a signalling response. Looking at the activity of proteins gives further insight into how these proteins relate to a particular condition, like depression. For this reason, in a recent study, we examined how IL-6 activity relates to symptoms and cognitive performance in people diagnosed with depression. (more…)
In a post first published on The Scholarly Kitchen blog, Nina Di Cara and Claire Haworth discuss the Data Hazards project and how it is being applied to improve how data ethics are identified and communicated in mental health research.(more…)
Éimear Foley discusses a new systematic review examining links between inflammation and depression.
Depression is an illness that is estimated to affect around 10-20% of the world’s population in a lifetime. However, for many people, current treatment strategies do not work sufficiently well. Depression is a multifactorial condition and there is mounting evidence that several biological and non-biological mechanisms may be at play.
One aetiological factor of increasing interest is inflammation. Prof Golam Khandaker, Head of the Immunopsychiatry Programme at the University of Bristol’s MRC Integrative Epidemiology Unit, tries to illustrate this point by asking people to think of the symptoms they experience when they have a cold or flu. Along with a runny nose and a cough, people often experience fatigue, a change to usual appetite or sleeping patterns, and/or a reduced ability to experience pleasure. He points out that these are also typical symptoms of major depressive disorder. Moreover, were you to have a blood sample taken, you would also find evidence of high levels of inflammation due to the activation of an immune response. Recent research suggests that up to a quarter of all depressed patients consistently show evidence of inflammation in their blood, as defined by C-reactive protein levels. Other studies have supported these findings, showing that depression may be causally linked to elevated concentrations of proinflammatory cytokines (i.e., proteins often used as markers of inflammation), like interleukin 6.
‘What do you think is most important for our health – our genetics or the environment we live in; nature or nurture?’
This was a key question that we posed to members of the public as part of a roundtable discussion on the topic of “Inherited Health”. We hosted our roundtable as part of the recent FUTURES public engagement festival and our event was attended by approximately 25 members of the public including retired professors, patent lawyers, and civil servants. (more…)
How do you feel about researchers tracking your mood using technology? How about tracking your physical activity or your sleep? How much technology will we let into our lives in the name of research?
These were the questions being asked this summer, when a team of researchers (from Bristol, Manchester, London and Oslo) went to speak to members of the public. They took the University of Bristol’s mobile lab around the city of Bristol and surrounding areas, to festivals, community groups and local parks. They wanted to understand public perceptions towards the use of technology to monitor mood and behaviour throughout the day, whether or not this was acceptable, and how to involve a diverse group of people in their research. In this blog post they tell us about what they did and what they found out. (more…)
Gemma Sharp and Flo Martin reflect on the importance of engaging with men, as well as women, when it comes to public engagement about menstruation and pregnancy research(more…)
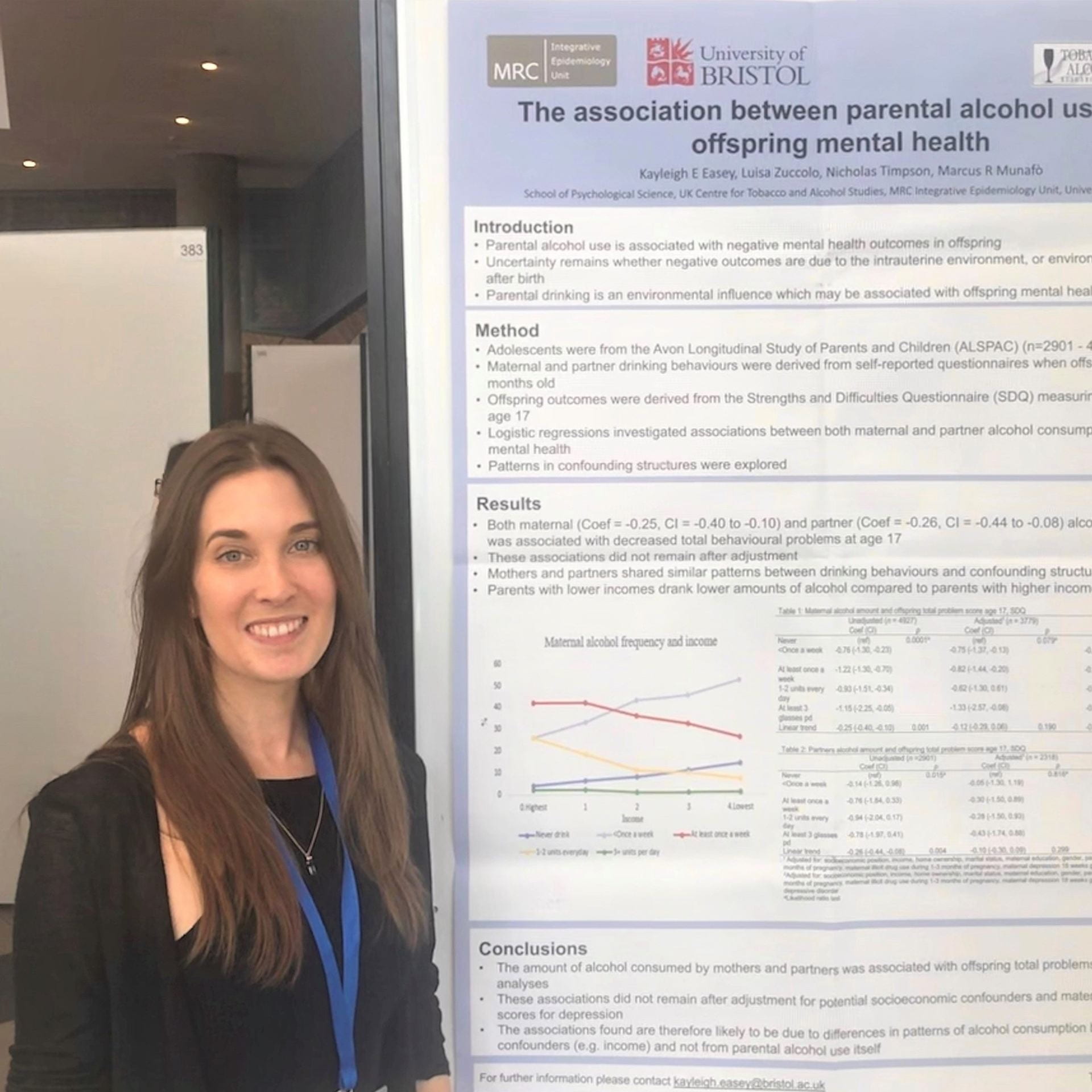
Dr Kayleigh Easey (@KayEasey), from the Bristol Medical School’s MRC Integrative Epidemiology Unit at the University of Bristol, takes a look at a recent research investigating effects of drinking in pregnancy and child mental health.
Whilst it’s generally known that heavy alcohol use during pregnancy can cause physical and cognitive impairments in offspring, there has been relatively limited evidence about the effects of low to moderate alcohol use. As such there have been conflicting conclusions about the potential harm of drinking in pregnancy, and debate around official guidance.
Alcohol use in pregnancy is still common with a recent meta-analysis showing over 40% of women within the UK to have drank some alcohol whilst pregnant. In 2016 the Department of Health updated their guidance advising abstinence from alcohol throughout pregnancy. This was in contrast to their previous advice of abstaining from alcohol in the first three months, but that 1-2 units of alcohol per week were not likely to cause harm. The updated guidance reflected a precautionary approach based on researcher’s advice of ‘absence of evidence not being evidence of absence’, due to the challenges faced in this area of study.
Certainly it has been challenging for researchers to determine any causal effect of alcohol use in pregnancy, particularly as the existing observational studies do not show evidence of causality. As such, caution over interpretation of results is needed given the sensitivity of alcohol as a risk factor and traditional attitudes towards low-level drinking.
Our new research sought to add to the limited body of evidence investigating causal effects, specifically on how low to moderate alcohol use could influence offspring mental health. We used data from a longitudinal birth cohort (the Avon Longitudinal Study of Parents and Children) which has followed pregnant mothers, their partners and their offspring since the 1990s, to investigate whether the frequency mothers and their partners drank alcohol during pregnancy was associated with offspring depression at age 18. We also included partner’s alcohol use in pregnancy (which is unlikely to have a direct biological effect on the developing fetus) and were able to examine if associations were likely to be causal, or due to shared confounding factors between parents such as socio-demographic factors.
We found that children whose mothers drank any alcohol at 18 weeks pregnancy may have up to a 17% higher risk of depression at age 18 compared to those mothers who did not drink alcohol. What was really interesting here is that we also investigated paternal alcohol use during pregnancy and did not find a similar association. This suggests that the associations seen with maternal drinking may be causal, rather than due to confounding by other factors (which might be expected to be similar between mothers and their partners). Many of the indirect factors that could explain the maternal effects are shared between mothers and partners (such as socio-demographic factors); despite this, we only found associations for mothers drinking.
These findings suggest evidence of a likely causal effect from alcohol consumption during pregnancy, and therefore evidence to support the updated government advice that the safest approach for alcohol use during pregnancy is for abstinence. This adds to other limited research on the effects of low level alcohol use in pregnancy. Whilst further research is needed, women can use this information to further inform their choices and help avoid risk from alcohol use both during pregnancy and as a precautionary measure when trying to conceive, as supported by the #Drymester campaign.
Our study highlights also the importance of including partner behaviours during pregnancy to aid in identifying causal relationships with offspring outcomes, and also because these may be important in their own right. I am currently working within the EPoCH project (Exploring Parental Influences on Childhood Health) which investigates whether and how both maternal and paternal behaviours might impact childhood health. In the meantime, it may be time for a further public health promotion highlighting that an alcohol-free pregnancy really is safer for children’s health.
Deborah Lawlor, Professor of Epidemiology, Emma Anderson, MRC Research Fellow, Marcus Munafò, Professor of Experimental Psychology, Mark Gibson, PhD student, Rebecca Richmond, Vice Chancellor’s Research Fellow
Association is not causation – are we fooled (confounded) when we see associations between sleep problems and disease?
Sleep is important for health. Observational studies show that people who report having sleep problems are more likely to be overweight, and have more health problems including heart disease, some cancers and mental health problems.
A major problem with conventional observational studies is that we cannot tell whether these associations are causal; does being overweight cause sleep problems, or do sleep problems cause people to become overweight? Alternatively, factors that influence how we sleep may also influence our health. For example, smoking might cause sleep problems as well as heart disease and so we are fooled (confounded) into thinking sleep problems cause heart disease when it is really all explained by smoking. In the green paper Advancing our Health: Prevention in the 2020s, the UK Government acknowledged that sleep has had little attention in policy, and that causality between sleep and health is likely to run in both directions.
But, how can we determine the direction of causality for sure? And, how do we make sure we are results are not confounded?
Randomly allocated genetic variation
Our genes are randomly allocated to us from our parents when we are conceived. They do not change across our lifespan, and cannot be changed by smoking, overweight or ill health.
Here at the MRC Integrative Epidemiology Unit we have developed a research method called Mendelian randomization, which uses this family-level random allocation of genes to explore causal effects. To find out more about Mendelian randomization take a look at this primer from the Director of the Unit (Prof George Davey Smith).
In the last two years, we and colleagues from the Universities of Manchester, Exeter and Harvard have identified large numbers of genetic variants that relate to different sleep characteristics. These include:
Insomnia symptoms
How long, on average, someone sleeps each night
Chronotype (whether someone is an ‘early bird’ or ‘lark’ and prefers mornings, or a ‘night owl’ and prefers evenings). Chronotype is thought to reflect variation in our body clock (known as circadian rhythms).
We can use these genetic variants in Mendelian randomization studies to get a better understanding of whether sleep characteristics affect health and disease.
What we did
In our initial studies we used Mendelian randomization to explore the effects of sleep duration, insomnia and chronotype on body mass index, coronary heart disease, mental health problems, Alzheimer’s disease, and breast cancer. We analysed whether the genetic traits that are related to sleep characteristics – rather than the sleep characteristics themselves – are associated with the health outcomes. We combined those results with the effect of the genetic variants on sleep traits which allows us to estimate a causal effect. Using genetic variants rather than participants’ reports of their sleep characteristics makes us much more certain that the effects we identify are not due to confounding or reverse causation.
Are you a night owl or a lark?
What we found
Our results show a mixed picture; different sleep characteristics have varying effects on a range of health outcomes.
Breast cancer was not influenced by insomnia, but appeared to increase with longer sleep duration.
None of these classical sleep traits have any influence on Alzheimer’s disease, though we found some suggestive evidence that daytime napping might decreased its risk.
Having better research evidence about the effects of sleep traits on different health outcomes means that we can give better advice to people at risk of specific health problems. For example, developing effective programmes to alleviate insomnia may prevent coronary heart disease and depression in those at risk. It can also help reduce worry about sleep and health, by demonstrating that some associations that have been found in previous studies are not likely to reflect causality.
If you are worried about your own sleep, the NHS has some useful guidance and signposting to further support.
Genome-wide association study identifies genetic loci for self-reported habitual sleep duration supported by accelerometer-derived estimates. Nature Comms. (2019) https://www.nature.com/articles/s41467-019-08917-4
Investigating causal relations between sleep traits and risk of breast cancer in women: mendelian randomisation study. BMJ (2019) https://www.bmj.com/content/365/bmj.l2327
Kayleigh Easey, a PhD student and member of the Tobacco and Alcohol Research Group (TARG) at the School of Psychological Science at the University of Bristol, takes a look at a recent systematic review investigating effects of parental alcohol use and offspring mental health.
It’s generally well known that drinking large amounts of alcohol during pregnancy is linked to Foetal Alcohol Syndrome (FAS), and negative outcomes such as premature birth and an increase in the risk of miscarriage. However, less is known about the effects of low to moderate alcohol use during pregnancy on offspring outcomes after birth, and even less for mental health outcomes in the child, particularly internalising disorders such as depression. Despite government guidelines being updated by the Department of Health in January 2016, advising pregnant women that the safest approach is to abstain from drinking alcohol altogether through their pregnancy, there remains uncertainty amongst the public as to whether a ‘drink or two’ is harmful or not.
Is a ‘drink or two’ harmful during pregnancy?
Researchers within the field mostly agree that abstinence from alcohol during pregnancy is the safest approach, but the evidence to support this is relatively weak, often due to study design and sample limitations. A previous meta-analysis highlighted how there are relatively few studies investigating low levels of alcohol use in pregnancy. Their analyses mainly focused on pregnancy outcomes such as gestational diabetes and childhood outcomes linked to FAS such as behavioural problems. Until now, a comprehensive review had not been undertaken on the effects of light to moderate drinking in pregnancy and offspring mental health.
Our research sought to review and summarise what literature was currently available for drinking alcohol in pregnancy and offspring mental health outcomes. Overall, we found that over half of the analyses included in the review reported an association between drinking in pregnancy and offspring mental health problems, specifically anxiety, depression, total problems and conduct disorder. By excluding FAS samples we were more certain that the findings we were reporting were representative of lower levels of drinking in pregnant women. However, we can’t be certain that many of the included studies are not still capturing higher levels of alcohol use in pregnancy, and potentially children with undiagnosed foetal alcohol spectrum disorders – a known problem in researching prenatal alcohol use.
Our review also highlights the differences across studies measuring drinking in pregnancy and offspring mental health, with all but four studies using a different measure of drinking alcohol in pregnancy, making comparison difficult. This means it is difficult to establish between studies if there is a ‘cut off’ level for what is potentially a hazardous level of alcohol exposure during pregnancy.
The associations we find do not provide evidence of a causal effect on their own, which can be difficult to demonstrate. However, it is important for women to understand what the current evidence shows, to allow them to make informed decisions about drinking during pregnancy. Women should be able to use this information to inform their choices, and to avoid potential risks from alcohol use, both during pregnancy and as a precautionary measure when trying to conceive.
As such, people may take from this that the current advice of abstaining from alcohol during pregnancy is certainly sensible, at least until evidence is available to indicate otherwise. We suggest that future work is needed to investigate whether light to moderate alcohol use in pregnancy may be harmful to different mental health outcomes in children from large cohort studies, which is exactly what I am currently doing within my PhD research using the Children of the 90s study.
Depression is one of the biggest public health challenges we’re currently facing and is expected to be the highest global burden of disease by 2030. The world health organisation (WHO) estimates that around 300 million people worldwide currently experience depression and that at least one in five people will experience depression at some stage of their life. Treatment is not always successful with only around 40-60% of individuals responding positively to antidepressant medication, and other forms of treatment such as cognitive behavioural therapy (CBT) or other talking based therapies requiring long waiting times of up to two years. It’s no surprise to see that depression and other mental health treatments are considered to be in a ‘crisis’ as we continually look for new and effective ways to combat this disease.
Research suggests that depression may first begin to manifest early in adolescence and young adulthood. This may have serious downstream consequences as depression during adolescence is related to both concurrent and later self-harm and suicide, corresponding mental health problems (like anxiety, addiction and psychosis) and impaired social functioning (reduced cognitive functioning and reclusiveness), to name a few. It also appears that depression during adolescence and young adulthood may actually be getting worse. Now whether or not this is because young people are talking more about their mental health than before remains to be seen, but that has not stopped researchers identifying potential causes for depression in adolescence in the hope of developing new and effective treatments and interventions. The message seems to be clear: by stopping/reducing depression in young people, we can potentially improve the quality of life later on.
What is responsible for depression in young people?
The lived experience of depression between young people differs from one person to the next, meaning there is no ‘one-size-fits-all’ approach. But with the help of research, we have begun to identify things that individuals experiencing depression have in common, that could be useful for treating and even preventing depression in young people. What follows is a whistle stop tour of some of the findings of potential causes of depression in young people.
Bullying
It may seem obvious, but childhood and adolescent bullying is one of the strongest predictors of current and later depression. One recent study found that individuals who had been bullied during adolescence were almost 3 times more likely to be depressed at age of 18. Bullying is particular prevalent during school years but can also occur well into the workplace or later education, which can have lasting effects on an individual’s mental health. Stopping bullying from occurring will be difficult, but that does not mean we cannot support individuals who have been bullied in order to help prevent depression from occurring or getting more severe.
Parental Depression
A lot of research has focused on the role of parental mood and later depression in young people. The role of parenting cannot be understated as numerous studies have shown that children of depressed parents are more likely to go on to have depression themselves, see research by Pearson et al,Stein et al and Gutierrez-Galve et al. However, it’s not clear if this is passed on genetically from the parent to child, or if there is something in the “environment” that transmits depression from parent to child. Whilst we don’t know for sure, the answer looks like it could be a bit of both. Parents may pass on depression genetically to their children, but depressed parents may also create an environment that makes the child more liable to depression. It is even possible that the parent passes on their genetics and the child then creates an environment for themselves that makes them more liable to depression. This is a form of gene-environment correlation that I won’t discuss in detail, but research is beginning to tease this apart with regard to parent and childhood depression.
Genetics
Interest in the genetics of depression has been heightened in the last few years. We always knew from twin studies that depression was likely to be heritable (i.e., that depression can be passed on from generation to generation), but convincing some that depression could have a strong genetic basis was tough (for a really good debate on this involving Professor Marcus Munafò, you can listen to this episode of BBC Start the Week). Most recently it has been shown that common genetic variants associated with depression in adulthood seem to predict greater levels of depression in children and adolescents, as well as varying patterns of depressive mood across adolescence. Importantly, it’s clear that there is no ‘one gene’ for depression. Instead, there are multiple genes which can be referred to as ‘polygenicity’ or ‘polygenic risk scores’; “poly” meaning multiple and “risk” indicating that individuals carrying multiple risk genes are more liable or ‘at risk’ to depression. By using polygenic risk scores we can begin to identify individuals experiencing depression early by using knowledge of their genetic make-up. However, it is really important to state here that genetic liability to depression does not equal genetic determinism. Just because someone is more genetically liable to depression, does not mean they will get depressed. There are multiple other factors at play, and we do not know how genetic liability to depression impacts on other pathways (i.e., does having genetic liability make you more likely to seek out an environment that could leave you more depressed?); but many researchers are beginning to ask these questions.
Taken together, these findings highlight how diverse depression is and how many factors could underlie depression in adolescence. There are a ton of other factors that have been related to adolescent depression that I have not had time/space to talk about. That is not to say they are not important, because most likely some are. As research develops and we are able to utilise different methods, we will get a better picture of what underpins depression in adolescence and what can be done to prevent and treat it.
What can we do?
Well for one, we have to keep up the research. We don’t know nearly enough about the underlying mechanisms and pathways that truly underlie adolescent depression. Researchers are beginning to examine this further with novel and promising techniques, but we also have to streamline the time it takes for research to be put into practise. The prolific mental health blog “The Mental Elf” states that it takes 17 years for research to reach clinical practise. That’s a long time and means a lot of people could miss out on the treatment they deserve.
Secondly, we have to be more forthright in how we talk about depression. You may have heard the expression ‘it is ok to be not be ok”. Avoiding telling people to “man-up” when they’re feeling depressed, speaking out and campaigns will only drive this forward. We have to normalise the fact that depression is a disease and like any other disease, it is good to talk about it. Only by talking about depression can we really move forward to end the stigma that being depressed is some kind of weakness. In fact one of my favourite instances of this recently was well explained by the England international Danny Rose.
Where do we go from here?
We appear to be reaching a turning point where more and more people are discussing mental health issues. This may be celebrities, royals or just your average Jo from down the street. But what is important is that we recognise the problem. That depression is a global burden that may be getting worse and requires our utmost attention and action. We are beginning to understand the causes of depression and how we might tackle it through research and reducing the social stigma that surrounds depression. However, the question is whether or not we can take advantage of these changes to really make a difference. Can we build on the progress we have made to finally one day beat depression? Yes. I really believe we can.
There are some awesome twitter feeds out there who I have always found to be really helpful and supportive of mental health issues. These people really get depression and are leading the charge in one way or another so do please give them a follow:
 These were the questions being asked this summer, when a team of researchers (from Bristol, Manchester, London and Oslo) went to speak to members of the public. They took the University of Bristol’s
These were the questions being asked this summer, when a team of researchers (from Bristol, Manchester, London and Oslo) went to speak to members of the public. They took the University of Bristol’s  Gemma Sharp and Flo Martin reflect on the importance of engaging with men, as well as women, when it comes to public engagement about menstruation and pregnancy research
Gemma Sharp and Flo Martin reflect on the importance of engaging with men, as well as women, when it comes to public engagement about menstruation and pregnancy research