‘What do you think is most important for our health – our genetics or the environment we live in; nature or nurture?’
This was a key question that we posed to members of the public as part of a roundtable discussion on the topic of “Inherited Health”. We hosted our roundtable as part of the recent FUTURES public engagement festival and our event was attended by approximately 25 members of the public including retired professors, patent lawyers, and civil servants. (more…)
Seed funding from Elizabeth Blackwell Institute enabled three researchers to develop their projects by including the ideas and experience of patients and the public. Article by Barney Marsh, originally published here. (more…)
How do you feel about researchers tracking your mood using technology? How about tracking your physical activity or your sleep? How much technology will we let into our lives in the name of research?
These were the questions being asked this summer, when a team of researchers (from Bristol, Manchester, London and Oslo) went to speak to members of the public. They took the University of Bristol’s mobile lab around the city of Bristol and surrounding areas, to festivals, community groups and local parks. They wanted to understand public perceptions towards the use of technology to monitor mood and behaviour throughout the day, whether or not this was acceptable, and how to involve a diverse group of people in their research. In this blog post they tell us about what they did and what they found out. (more…)
Gemma Sharp and Flo Martin reflect on the importance of engaging with men, as well as women, when it comes to public engagement about menstruation and pregnancy research(more…)
‘Enhancing the utilization of COVID-19 testing in schools’, is a study which will look at the characteristics of long COVID and COVID-19 infection in children. ‘Long COVID’ is commonly used to describe signs and symptoms that continue or develop after acute COVID‑19. The study is being funded as a result of a rapid funding call by Health Data Research UK (HDR UK), the Office for National Statistics (ONS) and UK Research and Innovation (UKRI). The study forms part of the larger Data and Connectivity National Core Study, which is led by HDR UK in partnership with ONS.
The COVID-19 testing in schools study is related to the CoMMinS (COVID-19 Mapping and Mitigation in Schools) study being undertaken by the University of Bristol in partnership with Bristol City Council, Public Health England [PHE] and Bristol schools. CoMMinS aims to give us an understanding of COVID-19 infection dynamics centred around school pupils and staff and onward transmission to family contacts, using regular testing. Our study will jointly analyse data from CoMMinS, along with information from Electronic Patient Records, and data from the COVID-19 Schools Infection Survey (SIS; jointly led by the London School of Hygiene & Tropical Medicine [LSHTM], PHE, and ONS). The SIS is a study similar to CoMMinS but carried out nationally.
To help inform research questions and methods for the study, members from the University of Bristol study team gathered views about long COVID in children between 9 March and 30 April 2021 from:
seven young people from the NIHR Bristol Biomedical Research Centre Young People’s Advisory Group (YPAG)
five families whose children have long COVID or suspected long COVID, recruited through two online UK campaign groups for long COVID, and
a survey completed by four GPs and one paediatrician, and an online meeting with two paediatricians.
It is important to note that the opinions gathered were based on small samples which may not be representative.
Through the meeting and survey with the doctors, the study team found that clinical understanding of long COVID in children is currently very limited.
The doctors said that it may be hard to distinguish between long COVID and other conditions with similar symptoms. Many of the symptoms of long COVID, like fatigue and feeling sick, aren’t very specific, and are common to many different conditions. Long COVID in children currently lacks a clinical definition, making diagnosis difficult. It isn’t yet properly understood whether long COVID is a new condition in itself, or a group of conditions like post viral fatigue, which is already recognised.
Young people, and families of children with long COVID or suspected long COVID, who were also asked for their opinion, said that feeling sick or stomach pain, extreme tiredness, and headaches were the symptoms they would rank as most ‘harmful’. For young people, this was based on them imagining having the symptoms. For the families, this was based on their first-hand experience.
The families also said that the symptoms their children were experiencing were numerous, often very severe, and more wide-ranging than those currently listed on the NHS website for long COVID. It is not yet clear what is causing the unusual symptoms.
The families said that they had struggled to get a diagnosis and treatment for their children. They also said that long COVID symptoms were having a significant impact on their children’s day-to-day lives both physically and psychologically, and that some of the children had missed school because of the symptoms. Some of the families also found fevers difficult to manage because their children had to miss school to self-isolate every time they had a fever. They wanted to know why the set of symptoms were being experienced, and why their children in particular had developed them.
It is not known how many children have or will develop long COVID. So far, studies which have tried to measure the rate of long COVID in children suggest it is rare. However, quantifying the number of cases is made difficult by a lack of clinical understanding of long COVID including the lack of an agreed clinical definition. The opinions collected suggest that relying on clinical diagnoses alone will under-estimate cases. On the other hand, there needs to be a cautious approach to estimating the number of cases based on non-specific symptoms, as other conditions which cause similar symptoms may be counted as well.
Caroline Relton, Professor of Epigenetic Epidemiology and Director of the Bristol Population Health Science Institute at the University of Bristol, joint lead for CoMMinS and one of the lead authors of the report, said: “The opinions we gathered further highlight that it is difficult to count the number of children with long COVID on the basis of diagnoses alone while long COVID in children remains poorly defined.
“There are added complications of studying long COVID in children, when it is sometimes difficult to disentangle what might be the result of experiencing infection from what might result from the wider impact of experiencing the pandemic. Isolation, school closures, disrupted education and other influences on family life could all have health consequences. Defining the extent of the problem in children and the root causes will be essential to helping provide the right treatment and to aid the recovery of young people who are suffering.”
The findings highlight that examining GP and hospital visits, and school attendance, might currently be a more useful and feasible way of assessing how COVID-19 has affected children, rather than relying only on diagnoses of long COVID. However, the study researchers also need to be aware how often healthcare is accessed according to need, and absence from school due to self-isolation, which will affect what is being measured.
Feeling sick or stomach pain, extreme tiredness, and headaches will be important symptoms to consider in the study.
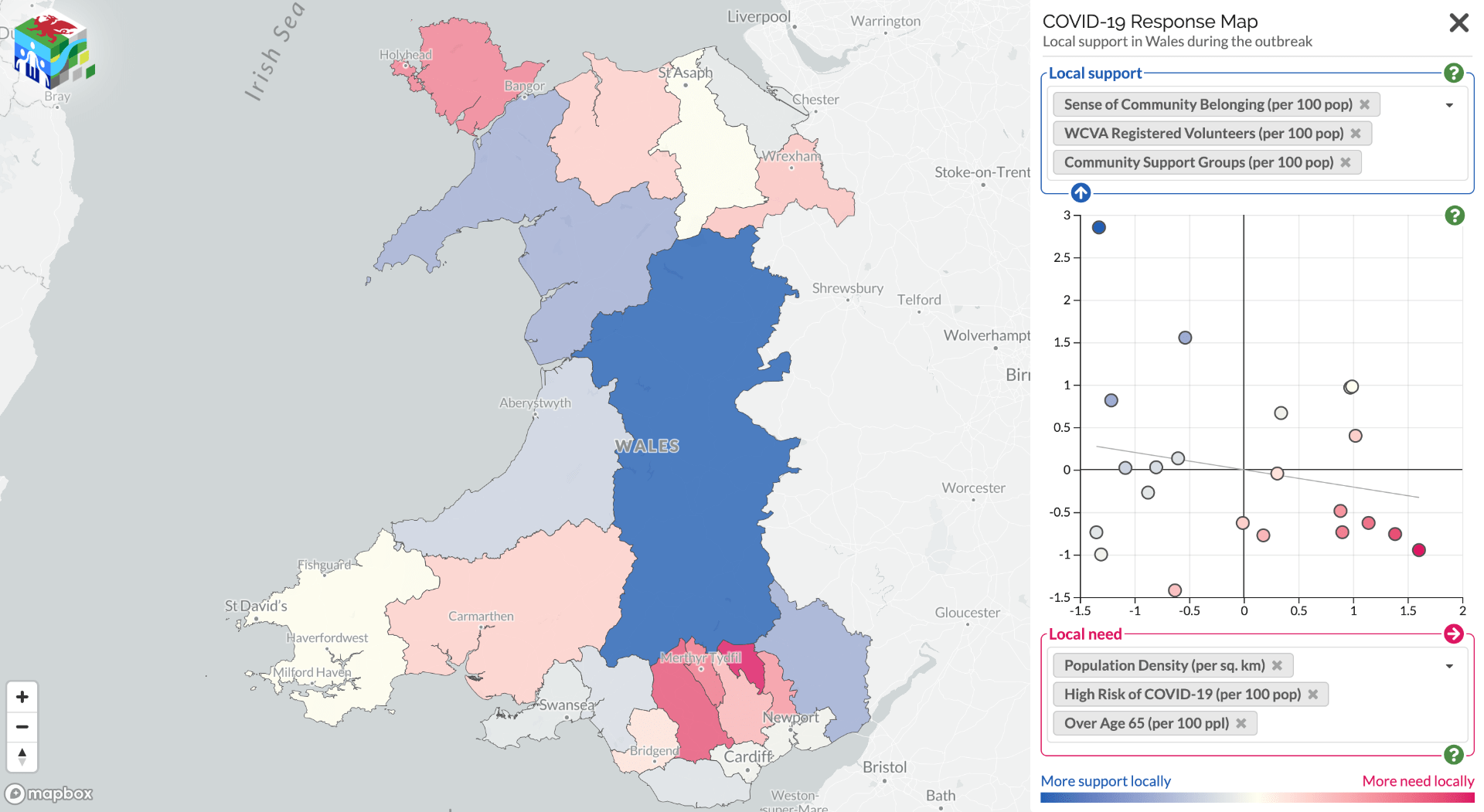
Since the pandemic started, communities have been mobilising to help each other; from shopping for elderly neighbours, to offering to offering a friendly face or other support. Mutual aid networks have sprung up all over the country, and neighbours who hadn’t previously spoken have been introduced to each other via street–level WhatsApp groups. But the degree to which offers of help are matching up with the need for help has been unknown, and this poses a problem for organisations who need to make decisions about where they should target limited resources.
Community support can offer a protective factor against adverse events. Some areas are more vulnerable than others, but knowing which areas are most likely to have a mismatch between support needed and support offered is difficult. To address this issue, a collaboration between the Public Health Wales Research & Evaluation Division and the Dynamic Genetics lab, part of the MRC Integrative Epidemiology Unit at the University of Bristol and supported by the Alan Turing Institute, has mapped these support offers and needs.
Using data from Wales Council for Voluntary Action, COVID-19 Mutual Aid, Welsh Government Statistics and Research, the Office for National Statistics, and social media the project team have created alive map that highlights the areas where further support for communities may be needed. It shows data on support factors, such as number of registered volunteers and population density, against risks, such as demographics, levels of deprivation, and internet access. It aims to inform the responses of national and local government, as well as support providers in Wales.
The site also provides the links to local community groups identified helping to raise awareness of the support available locally.
This map is part of an effort to better understand which communities have better community cohesion and organisation. We are keen to find out your views on how this can be more useful, or other community mobilisation data sources which could be included. Please contact Oliver or Nina with your comments:
If you are a community group and want to be included, please register your group with Covid-19 Mutual Aid (https://covidmutualaid.org/).
The code used to create the map has been released openly on GitHub (https://github.com/DynamicGenetics/COVID-19-Community-Response) so that it can be reproduced. Full information on the sources of data on vulnerability and community support are documented on the Open Science Framework (https://osf.io/c48hw/) and the map will be updated as new information becomes available.
Back in May, IEU researcher Dr Gemma Sharp took part in Creative Reactions, an initiative that pairs scientists with artists to create artwork based on their academic research. With 50 artists and 50 scientists collaborating on works from sculptures and wood carvings to canvas, digital and performance art, the 2019 exhibition ran across two venues in Bristol.
Gemma was paired with Olga Trevisan, an artist based in Venice, Italy. They had conversations over Skype where they spoke about their work and formed some initial ideas about how they could combine their interests in a new way while remaining coherent to their own practices. Reflecting on the collaboration, Olga said, “I love how curious you can be of a subject you haven’t considered before. I believe collaboration helps to open your own mind.”
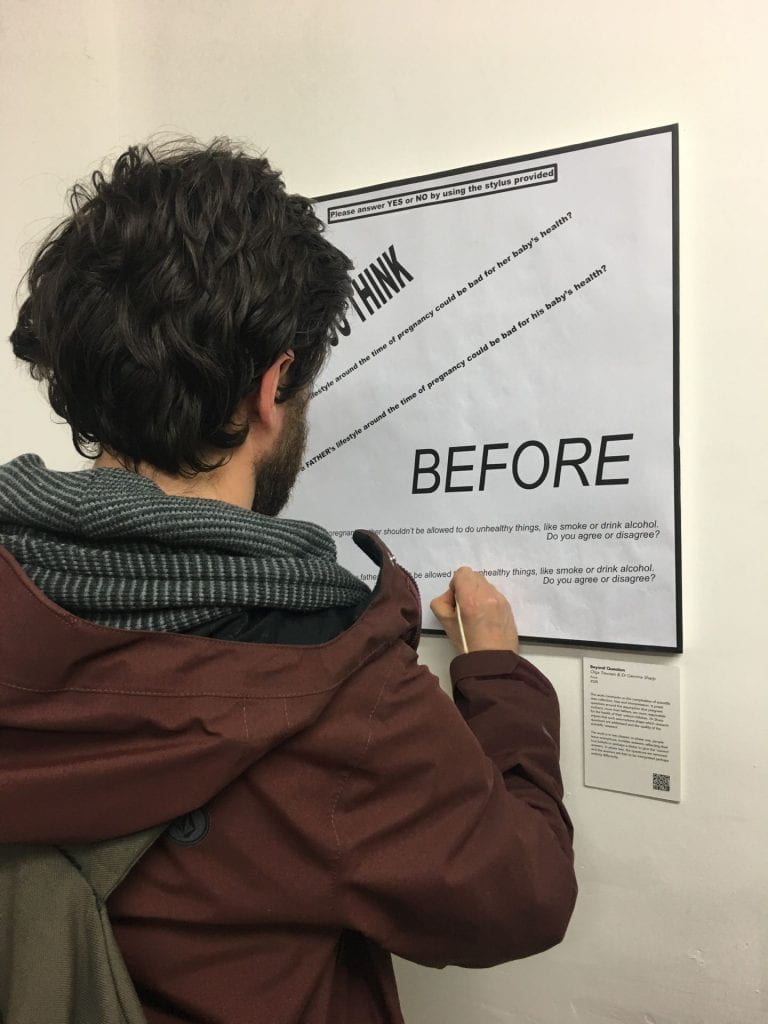
Based on some of the work around EPoCH, Olga created a piece called Beyond Question, which comments on the complexities of scientific data collection, bias and interpretation.
It poses questions around the pervasive assumption that pregnant women are more responsible for the (ill) health of their unborn children than their male partners are. Gemma and colleagues have argued that such assumptions drive the research agenda and the public perception of parental roles, by shaping which research questions get asked, which data are collected, and the quality of the scientific ‘answer’.
Photo credit: Olga Trevisan
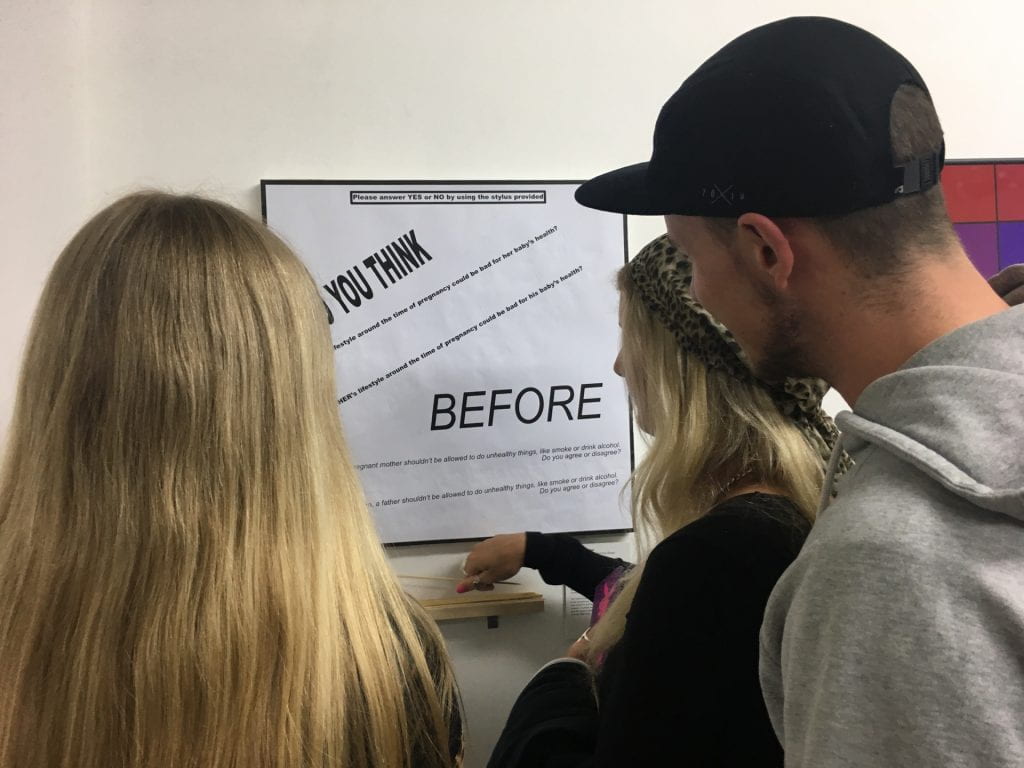
Beyond Question was presented in two phases at two separate exhibitions: during the first phase, people were invited to answer questions with a simple Yes or No using a stylus; leaving no marks but only invisible, anonymous traces on the surface below. Answers will reflect the real assumptions, beliefs and attitudes of the respondent, but perhaps also, despite anonymity, their eagerness to ‘please’ the questioners, to give the ‘right’ answer, and to mask their true responses to paint themselves in the ‘best’ light.
In the second phase, the questions were removed and the answer traces were left alone to carry their own meaning; free to be combined with the attitudes, beliefs and assumptions of the viewer and to be interpreted and judged in perhaps an entirely different way.
Photo credit: Olga Trevisan
The questions posed were:
“Do you think a mother’s lifestyle around the time of pregnancy could be bad for her baby’s health?”
“Do you think a father’s lifestyle around the time of pregnancy could be bad for his baby’s health?”
“Before her baby is born, a pregnant mother shouldn’t be allowed to do unhealthy things, like smoke or drink alcohol. Do you agree or disagree?”
“Before his baby is born, a father shouldn’t be allowed to do unhealthy things, like smoke or drink alcohol. Do you agree or disagree?”
Public health is one of the most contested policy areas. It brings together ethical and political issues and evidence on what works, and affects us all as citizens.
Researchers produce evidence and decision-makers receive advice – but how does evidence become advice and who are the players who take research findings and present advice to politicians and budget-holders?
We were pleased to welcome a diverse audience of around 75 multidisciplinary academics, policymakers and practitioners to hear our seminar speakers give a range of insider perspectives on linking academic research with national and local decisions on what to choose, fund and implement.
In this blog post we summarise the seminar, including links to the slides and event recording.
Seminar attendees in the Coutts lecture theatre. Image credit: Julio Hermosilla Elgueta
Chair David Buck from The King’s Fund opened the event, highlighting the importance of conversations between different sectors of the evidence landscape, and of local decision-making in this context.
‘The art of giving advice’
The session was kicked off by Richard Gleave, Deputy Chief Executive, Public Health England, who is also undertaking a PhD on how evidence is used in public health policy decision making.
His presentation ‘Crossing boundaries – undertaking knowledge informed public health’ set the context, observing that most academic teams – from microbiology labs to mental health researchers – aim to improve policy and practice; but ‘the art of giving advice is as important and challenging as the skill required to review the evidence’.
Richard then introduced a range of provocations and stereotypes about how the policy decision making process can be framed.
Citing Dr Kathryn Oliver, he encouraged attendees to challenge the idea that there’s an ‘evidence gap’ to be crossed, and instead focus on doing good working together to improve the public’s health.
Giving an example of the Institute for Government’s analysis of how the smoking ban was enacted, he noted the role of a small number of influential groups and individuals in securing a total ban in 2007. He encouraged actively crossing the boundaries between academia, policy and practice, and working with boundary organisations and influencers as part of this process.
‘Partnerships between science and society’
Professor Isabel Oliver gave a second national perspective.
Speaking as a research-active Director of Research, Translation and Innovation and Deputy Director of the National Infection Service, she suggested that ‘Partnerships between Science and Society’ are the key to evidence based public health.
She questioned why is it when we have such an abundance of research, we still don’t have the evidence we need? And why does it take so long to implement research findings? She argued that a key issue here is relevance; how relevant is the research being produced, especially to current policy priorities?
Isabel outlined challenges including:
Needing evidence quickly in response to public health emergencies, and not being able to access it, for example how to bottle-feed babies during flooding crises, or whether to close schools during flu pandemics
Mismatched policy and research priorities; e.g. policy needing evidence on the impact of advertising on childhood obesity, but research focusing on the genetics of obesity
The (unhelpful) prevalence of ‘more research needed’ as a conclusion, and knowing when the evidence is sufficient to make a decision
A need to develop trust between stakeholders, made more challenging by the frequency of policy colleagues moving roles.
She also questioned whether the paradigm of evidence-based medicine works for complex issues such as public health or environmental policy.
Isabel concluded with some observations; that broader and more collaborative research questions that address the real issues are needed; and collaborating with a broad range of stakeholders, including industry and finance, should not be discounted.
She finished by reiterating a call for public health advice that is relevant, and responds to a policy ‘window’ being open.
Seminar speakers L-R: Dr Olivia Maynard, Richard Gleave, Professor Isabel Oliver and Christina Gray. Image credit: Julio Hermosilla Elgueta
‘Local perspective’
Christina Gray, Director of Public Health at Bristol City Council gave the local view, providing a helpful explanation of her role and the process of decision making within a local authority.
She outlined three key principles:
The democratic principle; elected members are ‘the council’; officers (including her role) provide advice. Local authorities are close to their people and are publicly accountable. Their decisions are formally scrutinised and need to be justified, and resource allocation is a key – and stark – challenge, especially in the context of austerity.
The narrative principle: how the society that the authority represents holds multiple legitimate (and competing or conflicting) perspectives and realities, which all need to be considered.
The (social) scientific principle; the development of human knowledge in a systematic way – which is then shared into the democratic process, as one of a range of narratives.
Christina outlined a case study example of an initiative on period dignity which Bristol City Council is leading as part of Bristol’s One City Plan, and how the evidence base for the programme was located and used. She posed the question of what evidence matters locally, and suggested that evidence of impact, economic evidence, and retrospective evidence that demonstrates whether what has been done works, in order to build on it, are the most helpful. To close, Christina highlighted the importance of being ‘paradigm literate’ in order to navigate the complexity of public health decision making.
Academic perspective
Our final speaker, Dr Olivia Maynard, gave an academic perspective on how to advise decision makers.
Focusing on practical tips, she outlined her own work on tobacco, smoking, e-cigarettes, alcohol and other drugs and how she has engaged with various opportunities to work with policymakers.
Starting with a clear case for doing the work (it’s important, it’s interesting, to create impact), she went on to outline methods of engagement:
Proactively presenting your work; introduce yourself to policymakers interested in your area such as MPs, Peers, APPGs, subject specialists in parliamentary research services, advocacy groups, and PolicyBristol; review Hansard and Early Day Motions; get involved in parliamentary events
Respond to calls for evidence (University of Bristol researchers can find curated opportunities via the PolicyBristol PolicyScan)
Work directly with policymakers, for example via Policy Fellowships (for example with POST)
Olivia outlined some reflections around the differences between academia and policymaking.
Timelines for action is one, but she also used the changes towards plain packaging as an example to note that the policymaking process can span numerous years, presenting many opportunities for intervention.
She referred back to Christina’s point about ‘multiple competing realities’ to highlight that evidence is one of many factors to consider in policymaking.
She also encouraged academics to challenge ‘imposter syndrome’, by emphasising ‘you are more of an expert than you think you are’, and needing to make yourself known to be offered opportunities.
Where next?
Chair David Buck highlighted a number of themes running throughout the presentations including recognising the paradigms used by different stakeholders; questioning what counts as evidence, and being able to provide advice from an uncertain evidence base; and what these themes mean for all of us (and how willing are we to act on these reflections?)
The seminar concluded with a facilitated Q&A session spanning topics such as:
Should all research which influences policy be coproduced with user groups and policymakers?
What kind of ‘payback’ do stakeholder organisations need for their involvement in research projects?
How should researchers develop the skills needed to cross boundaries?
What funding is available for policy relevant research?
How can we make our evidence ‘stand out’?
Should academics have a responsibility to critique policy?
The seminar started numerous conversations which we hope to continue.
Chair David Buck facilitates our Q&A. Image credit: Julio Hermosilla Elgueta
The Green Paper on preventing ill health was published earlier this week, and many have criticised that proposals do not go far enough. Our guest blog explores some of the challenges that Public Health England face in providing evidence-informed advice. Read on to discover the reflections from a recent workshop on using evidence to influence local and national strategy and their implications for academic engagement with policymakers.
On the 12th June, at the invitation of Richard Gleave, Professor Paul Cairney and Dr John Boswell led a discussion on ‘institutionalising’ preventive health with senior members of Public Health England (PHE).
It follows a similar event in Scotland, to inform the development of Public Health Scotland, and the PHE event enjoyed contributions from key members of NHS Health Scotland.
This post summarises their presentation and reflections from the workshop (gathered using the Chatham House rule).
The Academic Argument
Governments face two major issues when they try to improve population health and reduce health inequalities:
Should they ‘mainstream’ policies – to help prevent ill health and reduce health inequalities – across government and/ or maintain a dedicated government agency?
Should an agency ‘speak truth to power’ and seek a high profile to set the policy agenda?
Our research provides three messages to inform policy and practice:
When governments have tried to mainstream ‘preventive’ policies, they have always struggled to explain what prevention means and reform services to make them more preventive than reactive.
Public health agencies could set a clearer and more ambitious policy agenda. However, successful agencies keep a low profile and make realistic demands for policy change. In the short term, they measure success according to their own survival and their ability to maintain the positive attention of policymakers.
Advocates of policy change often describe ‘evidence based policy’ as the answer. However, a comparison between (a) specific tobacco policy change and (b) very general prevention policy shows that the latter’s ambiguity hinders the use of evidence for policy. Governments use three different models of evidence-informed policy. These models are internally consistent but they draw on assumptions and practices that are difficult to mix and match. Effective evidence use requires clear aims driven by political choice.
Overall, they warn against treating any response – (a) the idiom ‘prevention is better than cure’, (b) setting up a public health agency, or (c) seeking ‘evidence based policy’ – as a magic bullet.
Major public health changes require policymakers to define their aims, and agencies to endure long enough to influence policy and encourage the consistent use of models of evidence-informed policy. To do so, they may need to act like prevention ninjas, operating quietly and out of the public spotlight, rather than seeking confrontation and speaking truth to power.
Image By Takver from Australia [CC BY-SA 2.0 (https://creativecommons.org/licenses/by-sa/2.0)], via Wikime
The Workshop Discussion
The workshop discussion highlighted an impressive level of agreement between the key messages of the presentation and the feedback from most members of the PHE audience.
One aspect of this agreement was predictable, since Boswell et al’s article describes PHE as a relative success story and bases its analysis of prevention ‘ninjas’ on interviews with PHE staff.
However, this strategy is subject to frequent criticism. PHE has to manage the way it communicates with multiple audiences, which is a challenge in itself. One key audience is a public health profession in which most people see their role as to provoke public debate, shine a light on corporate practices (contributing to the ‘commercial determinants of health’), and criticise government inaction. In contrast, PHE often seeks to ensure that quick wins are not lost, must engage with a range of affected interests, and uses quiet diplomacy to help maintain productive relationships with senior policymakers. Four descriptions of this difference in outlook and practice stood out:
Walking the line. Many PHE staff gauge how well they are doing in relation to the criticism they receive. Put crudely, they may be doing well politically if they are criticised equally by proponents of public health intervention and vocal opponents of the ‘nanny state’.
Building and maintaining relationships. PHE staff recognise the benefit of following the rules of the game within government, which include not complaining too loudly in public if things do not go your way, expressing appreciation (or at least a recognition of policy progress) if they do, and being a team player with good interpersonal skills rather than simply an uncompromising advocate for a cause. This approach may be taken for granted by interest groups, but tricky for public health researchers who seek a sense of critical detachment from policymakers.
Managing expectations. PHE staff recognise the need to prioritise their requirements from government. Phrases such as ‘health in all policies’ often suggest the need to identify a huge number of crucial, and connected, policy changes. However, a more politically feasible strategy is to identify a small number of discrete priorities on which to focus intensely.
Linking national and local. PHE staff who work closely with local government, the local NHS, and other partners, described how they can find it challenging to link ‘place-based’ and ‘national policy area’ perspectives. Local politics are different from national politics, though equally important in implementation and practice.
There was also high agreement on how to understand the idea of ‘evidence based’ or ‘evidence informed’ policymaking (EBPM). Most aspects of EBPM are not really about ‘the evidence’. Policy studies often suggest that, to improve evidence use requires advocates to:
find out where the action is, and learn the rules and language of debate within key policymaking venues, and
engage routinely with policymakers, to help them understand their audience, build up trust based on an image of scientific credibility and personal reliability, and know when to exploit temporary opportunities to propose policy solutions.
To this we can add the importance of organisational morale and a common sense of purpose, to help PHE staff operate effectively while facing unusually high levels of external scrutiny and criticism. PHE staff are in the unusual position of being (a) part of the meetings with ministers and national leaders, and (b) active at the front-line with professionals and key publics.
In other words, political science-informed policy studies, and workshop discussions, highlighted the need for evidence advocates to accept that they are political actors seeking to win policy arguments, not objective scientists simply seeking the truth. Scientific evidence matters, but only if its advocates have the political skills to know how to communicate and when to act.
Although there was high agreement, there was also high recognition of the value of internal reflection and external challenge. In that context, one sobering point is that, although PHE may be relatively successful now (it has endured for some time), we know that government agencies are vulnerable to disinvestment and major reform. This vulnerability underpins the need for PHE staff to recognise political reality when they pursue evidence-informed policy change. Put bluntly, they often have to strike a balance between two competing pressures – being politically effective or insisting on occupying the moral high ground – rather than assuming that the latter always helps the former.
Policy engagement is becoming more of a priority in academic life, as emphasis shifts from focusing purely on academic outputs to creating impact from research. Research impact is defined by UKRI as ‘the demonstrable contribution that excellent research makes to society and the economy’.
On 25 June 2019 the IEU held its first Engagers’ Lunch event, which focused on policy engagement. Joined by Dr Alisha Davies, Head of Research from Public Health Wales, Dr Laura Howe, Professor Debbie Lawlor and Dr Lindsey Pike from the IEU facilitated discussion drawing on their experiences – from both sides of the table – of connecting research and policy. Below we summarise advice from our speakers about engaging with policy.
The benefits of engaging with policy & how to do it
As an academic you need to consider what your ‘offer’ is. What expertise do you bring? This may be topic specific knowledge or relate to strong academic skills such as critical approaches to complex challenges, novel methods in evaluation, health economics. Recognise where you add value; the remit of academia is to develop robust evidence in response to complex and challenging questions using reliable methods – a gap that those in practice and /or policy cannot fill alone.
Find the right people to engage with – who are the decision makers in your area of research? Listen to what is currently important to inform action / policy. Read through local and national strategies in your topic of expertise to understand the wider landscape and where your work might inform, or where you might be able to address some of those key gaps. Academics can also submit evidence to policy (colleagues from the University of Bristol can access PolicyBristol’s policy scan, which lists current opportunities to engage).
Be visible and actively engage. Find out what local events are going on in your area related to your research and go along to meet local public health professionals. It’s a good way to meet people, find commonalities and form collaborations.
Condense your new research into a short briefing, identify what it adds to the existing evidence base, how does it inform given the wider context.
As an academic you will have a network of other research colleagues. Policymakers value being able to draw on this network for information. When providing evidence, don’t just cite your own – objectivity is one of the key advantages of working with academics, and policymakers value your intellectual independence. Your knowledge of the broader evidence base is invaluable.
Setting up a research steering group or stakeholder panel can be a great way to develop your relationships and ensure your research is speaking to policy, practice or industry priorities. Key to this is getting the right people involved – this blog post from Fast Track Impact has some useful advice.
The challenges of engaging with policy & how to navigate them
Academic and policymaking timescales are different. Policymakers need an answer yesterday while academics may not feel comfortable with providing a definitive response without time for reflection. There’s a need for flexibility on both sides.
There are also tensions between the perceived need for certainty and ability to be able to provide it. Policymakers may want ‘an answer’, but the evidence base may not be robust enough to give one. It is more useful to outline what we do and do not know, with a ‘balance of probabilities’ recommendation, than to say ‘more research is needed’.
Language can also be a barrier. Academic language is complex and, at times, impenetrable; policymaker documents need to be aimed at an intelligent lay audience, without jargon, and focusing on what matters to them (outlining policy options and the evidence base behind them – not lengthy discussions of statistical methods). Look at Public Health Wales’ publications, for example on digital technology, adverse childhood experiences and resilience, or mass unemployment events, or examples from the NIHR Dissemination Centre or PolicyBristol to get a sense of the language to use.
Do you think you have time for networking with non-academic stakeholders? The perception of opportunity costs can be another barrier for academics. While time for networking might not be costed into your grant funding, think of it in the same way as writing a grant application; you can’t guarantee the outcome but the potential reward is significant.
There are no guarantees in policy engagement work, and a level of realism is required around what findings from one study can achieve. Policymaking is a complex and messy process; the evidence base is just one factor in decision making. Your recommendations may not be taken up because of politics, resource issues, or other concerns taking priority. Sometimes your relationships will reach honourable dead ends, where you realise that interests, capacity or timescales are not as aligned as you thought. Knowing this before you start is important to avoid feeling disillusioned.
Policymaking is a complex and messy process; the evidence base is just one factor in decision making. Image from Sausages, evidence and policymaking: The role of universities in a post-truth world, Policy Institute at Kings 2017
In summary, the panel concluded that policymakers are interested in academic research as long as their priorities are addressed. While outcomes are not guaranteed, our colleagues at PolicyBristol advise a strategy of ‘engineered serendipity’ – looking for and capitalising on opportunities, being ready to talk about your research in a clear and policy orientated way (why does your research matter and what are the key recommendations?) and aim to build long term and trusting relationships with policymakers.
If you’d be interested in attending a future Engagers’ Lunch, please contact Lindsey Pike.
Further information & resources
PolicyBristolaims to enhance the influence and impact of research from across the University of Bristol on policy and practice at the local, national and international level.
Public Health Wales Research and Evaluation work collaboratively across Public Health Wales and with external academic and partner organisations, and are keen to facilitate research links across Public Health Wales with new national and international partners.
Parliamentary research services across the legislatures include:
House of Commons Library: an independent research and information unit. It provides impartial information for Members of Parliament of all parties and their staff.
Research and Information Service (RaISe): aims to meet the information needs of the Northern Ireland Assembly Members, their staff and the secretariat in an impartial, objective, timely and non-partisan manner.
Senedd Research: an expert, impartial and confidential research and information service designed to meet the needs of Wales’ National Assembly Members and their staff.
 These were the questions being asked this summer, when a team of researchers (from Bristol, Manchester, London and Oslo) went to speak to members of the public. They took the University of Bristol’s
These were the questions being asked this summer, when a team of researchers (from Bristol, Manchester, London and Oslo) went to speak to members of the public. They took the University of Bristol’s  Gemma Sharp and Flo Martin reflect on the importance of engaging with men, as well as women, when it comes to public engagement about menstruation and pregnancy research
Gemma Sharp and Flo Martin reflect on the importance of engaging with men, as well as women, when it comes to public engagement about menstruation and pregnancy research