Kayleigh Easey, a PhD student and member of the Tobacco and Alcohol Research Group (TARG) at the School of Psychological Science at the University of Bristol, takes a look at a recent systematic review investigating effects of parental alcohol use and offspring mental health.
It’s generally well known that drinking large amounts of alcohol during pregnancy is linked to Foetal Alcohol Syndrome (FAS), and negative outcomes such as premature birth and an increase in the risk of miscarriage. However, less is known about the effects of low to moderate alcohol use during pregnancy on offspring outcomes after birth, and even less for mental health outcomes in the child, particularly internalising disorders such as depression. Despite government guidelines being updated by the Department of Health in January 2016, advising pregnant women that the safest approach is to abstain from drinking alcohol altogether through their pregnancy, there remains uncertainty amongst the public as to whether a ‘drink or two’ is harmful or not.
Is a ‘drink or two’ harmful during pregnancy?
Researchers within the field mostly agree that abstinence from alcohol during pregnancy is the safest approach, but the evidence to support this is relatively weak, often due to study design and sample limitations. A previous meta-analysis highlighted how there are relatively few studies investigating low levels of alcohol use in pregnancy. Their analyses mainly focused on pregnancy outcomes such as gestational diabetes and childhood outcomes linked to FAS such as behavioural problems. Until now, a comprehensive review had not been undertaken on the effects of light to moderate drinking in pregnancy and offspring mental health.
Our research sought to review and summarise what literature was currently available for drinking alcohol in pregnancy and offspring mental health outcomes. Overall, we found that over half of the analyses included in the review reported an association between drinking in pregnancy and offspring mental health problems, specifically anxiety, depression, total problems and conduct disorder. By excluding FAS samples we were more certain that the findings we were reporting were representative of lower levels of drinking in pregnant women. However, we can’t be certain that many of the included studies are not still capturing higher levels of alcohol use in pregnancy, and potentially children with undiagnosed foetal alcohol spectrum disorders – a known problem in researching prenatal alcohol use.
Our review also highlights the differences across studies measuring drinking in pregnancy and offspring mental health, with all but four studies using a different measure of drinking alcohol in pregnancy, making comparison difficult. This means it is difficult to establish between studies if there is a ‘cut off’ level for what is potentially a hazardous level of alcohol exposure during pregnancy.
The associations we find do not provide evidence of a causal effect on their own, which can be difficult to demonstrate. However, it is important for women to understand what the current evidence shows, to allow them to make informed decisions about drinking during pregnancy. Women should be able to use this information to inform their choices, and to avoid potential risks from alcohol use, both during pregnancy and as a precautionary measure when trying to conceive.
As such, people may take from this that the current advice of abstaining from alcohol during pregnancy is certainly sensible, at least until evidence is available to indicate otherwise. We suggest that future work is needed to investigate whether light to moderate alcohol use in pregnancy may be harmful to different mental health outcomes in children from large cohort studies, which is exactly what I am currently doing within my PhD research using the Children of the 90s study.
Policy engagement is becoming more of a priority in academic life, as emphasis shifts from focusing purely on academic outputs to creating impact from research. Research impact is defined by UKRI as ‘the demonstrable contribution that excellent research makes to society and the economy’.
On 25 June 2019 the IEU held its first Engagers’ Lunch event, which focused on policy engagement. Joined by Dr Alisha Davies, Head of Research from Public Health Wales, Dr Laura Howe, Professor Debbie Lawlor and Dr Lindsey Pike from the IEU facilitated discussion drawing on their experiences – from both sides of the table – of connecting research and policy. Below we summarise advice from our speakers about engaging with policy.
The benefits of engaging with policy & how to do it
As an academic you need to consider what your ‘offer’ is. What expertise do you bring? This may be topic specific knowledge or relate to strong academic skills such as critical approaches to complex challenges, novel methods in evaluation, health economics. Recognise where you add value; the remit of academia is to develop robust evidence in response to complex and challenging questions using reliable methods – a gap that those in practice and /or policy cannot fill alone.
Find the right people to engage with – who are the decision makers in your area of research? Listen to what is currently important to inform action / policy. Read through local and national strategies in your topic of expertise to understand the wider landscape and where your work might inform, or where you might be able to address some of those key gaps. Academics can also submit evidence to policy (colleagues from the University of Bristol can access PolicyBristol’s policy scan, which lists current opportunities to engage).
Be visible and actively engage. Find out what local events are going on in your area related to your research and go along to meet local public health professionals. It’s a good way to meet people, find commonalities and form collaborations.
Condense your new research into a short briefing, identify what it adds to the existing evidence base, how does it inform given the wider context.
As an academic you will have a network of other research colleagues. Policymakers value being able to draw on this network for information. When providing evidence, don’t just cite your own – objectivity is one of the key advantages of working with academics, and policymakers value your intellectual independence. Your knowledge of the broader evidence base is invaluable.
Setting up a research steering group or stakeholder panel can be a great way to develop your relationships and ensure your research is speaking to policy, practice or industry priorities. Key to this is getting the right people involved – this blog post from Fast Track Impact has some useful advice.
The challenges of engaging with policy & how to navigate them
Academic and policymaking timescales are different. Policymakers need an answer yesterday while academics may not feel comfortable with providing a definitive response without time for reflection. There’s a need for flexibility on both sides.
There are also tensions between the perceived need for certainty and ability to be able to provide it. Policymakers may want ‘an answer’, but the evidence base may not be robust enough to give one. It is more useful to outline what we do and do not know, with a ‘balance of probabilities’ recommendation, than to say ‘more research is needed’.
Language can also be a barrier. Academic language is complex and, at times, impenetrable; policymaker documents need to be aimed at an intelligent lay audience, without jargon, and focusing on what matters to them (outlining policy options and the evidence base behind them – not lengthy discussions of statistical methods). Look at Public Health Wales’ publications, for example on digital technology, adverse childhood experiences and resilience, or mass unemployment events, or examples from the NIHR Dissemination Centre or PolicyBristol to get a sense of the language to use.
Do you think you have time for networking with non-academic stakeholders? The perception of opportunity costs can be another barrier for academics. While time for networking might not be costed into your grant funding, think of it in the same way as writing a grant application; you can’t guarantee the outcome but the potential reward is significant.
There are no guarantees in policy engagement work, and a level of realism is required around what findings from one study can achieve. Policymaking is a complex and messy process; the evidence base is just one factor in decision making. Your recommendations may not be taken up because of politics, resource issues, or other concerns taking priority. Sometimes your relationships will reach honourable dead ends, where you realise that interests, capacity or timescales are not as aligned as you thought. Knowing this before you start is important to avoid feeling disillusioned.
Policymaking is a complex and messy process; the evidence base is just one factor in decision making. Image from Sausages, evidence and policymaking: The role of universities in a post-truth world, Policy Institute at Kings 2017
In summary, the panel concluded that policymakers are interested in academic research as long as their priorities are addressed. While outcomes are not guaranteed, our colleagues at PolicyBristol advise a strategy of ‘engineered serendipity’ – looking for and capitalising on opportunities, being ready to talk about your research in a clear and policy orientated way (why does your research matter and what are the key recommendations?) and aim to build long term and trusting relationships with policymakers.
If you’d be interested in attending a future Engagers’ Lunch, please contact Lindsey Pike.
Further information & resources
PolicyBristolaims to enhance the influence and impact of research from across the University of Bristol on policy and practice at the local, national and international level.
Public Health Wales Research and Evaluation work collaboratively across Public Health Wales and with external academic and partner organisations, and are keen to facilitate research links across Public Health Wales with new national and international partners.
Parliamentary research services across the legislatures include:
House of Commons Library: an independent research and information unit. It provides impartial information for Members of Parliament of all parties and their staff.
Research and Information Service (RaISe): aims to meet the information needs of the Northern Ireland Assembly Members, their staff and the secretariat in an impartial, objective, timely and non-partisan manner.
Senedd Research: an expert, impartial and confidential research and information service designed to meet the needs of Wales’ National Assembly Members and their staff.
Every two years my department puts on a conference on the topic of Mendelian Randomization (MR), a field that has been pioneered by researchers in Bristol over the last two decades. After months of planning, including finding a venue, inviting speakers from around the world and arranging the scientific programme, it’s a week and a half to go and we’re almost there!
But what is Mendelian Randomization research all about I hear you ask? Are you sure you want to know? Please read on but understand there is no going back…..
Are you sure you want to know about Mendelian Randomisation?
Have you ever had the feeling that something wasn’t quite right, that you are being controlled in some way by a higher force?
Well, it’s true. We are all in The Matrix. Like it or not, each of us has been recruited into an experiment from the moment we were born. Our genes, which are given to us by our parents at the point of conception, influence every aspect of our lives: how much we eat, sleep, drink, weigh, smoke, study, worry and play. The controlling effect is cleverly very small, and scientists only discovered the pattern by taking measurements across large populations, so as individuals we generally don’t notice. But the effect is real, very real!
How can we fight back?
We cannot escape The Matrix, but we can fight back by extracting knowledge from this unfortunate experiment we find ourselves in and using it for society’s advantage. For example, if we know that our genes predict 1-2% of variation in Low-Density Lipoprotein cholesterol (LDL-c – the ‘bad’ cholesterol) in the population, we can see if genes known to predict LDL-c also predict later life health outcomes in a group of individuals such as an increased risk of heart disease. If they do, then it provides strong evidence that reducing LDL-c will reduce heart disease risk, and we can then take steps to act. This is, in essence, the science of Mendelian randomization. See here for a nice animation of the method by our Unit director, George Davey Smith – our Neo if you like.
An example of the mathematical framework that leads to our analysis (honest)
Mendelian randomization is very much a team effort, involving scientists with expertise across many disciplines. My role, as a statistician and data scientist is to provide the mathematical framework to ensure the analysis is performed in a rigorous and reliable manner.
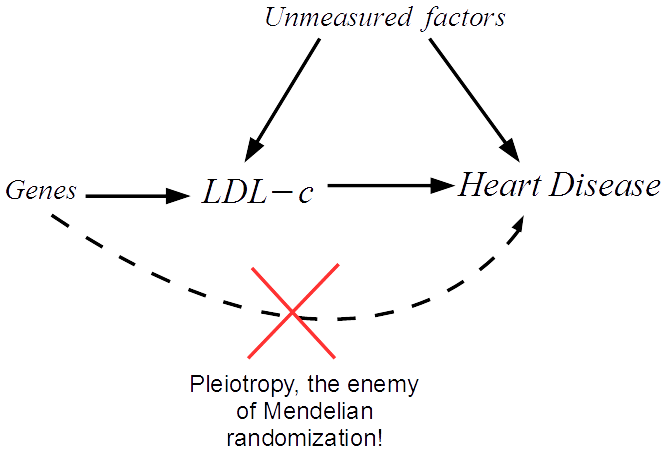
We start by drawing a diagram that makes explicit the assumptions our analysis rests on. The arrows show which factors influence which. In our case we must assume that a set of genes influence LDL-c, and can only influence heart disease risk through LDL-c. We can then translate this diagram into a system of equations that we apply to our data.
The great thing about Mendelian randomization is that, even when many other factors jointly influence LDL-c and heart disease risk, the Mendelian randomization approach should still work.
Recently, the validity of the Mendelian randomization approach has been called into question due to the problem of pleiotropy. In our example this would be when a gene affects heart disease through a separate unmodelled pathway.
An illustration of pleitropy
This can lead to bias in the analysis and therefore misleading results. My research is focused on novel methods that try to overcome the issue of pleiotropy, by detecting and adjusting for its presence in the analysis. For further details please see this video.
The MR Data challenge
At this year’s conference we are organising an MR Data Challenge, to engage conference participants in exploring and developing innovative approaches to Mendelian randomization using a publicly available data set. At a glance, the data comprises information on 150 genes and their association with
118 lipid measurements (LDL cholesterol)
7 health outcomes (including type II diabetes)
Eight research teams have submitted an entry to the competition, to describe how they would analyse the data and the conclusions they would draw. The great thing about these data is that the information on all 118 lipid traits simultaneously assessed to improve the robustness of the Mendelian randomization analysis.
Genetic data can help us understand how to resolve population health issues. Image credit: www.genome.gov
A key aim of the session is to bring together data scientists with experts from the medical world to comment on and debate the results. We will publish all of the computer code online so that anyone can re-run the analyses. In the future, we hope to add further data to this resource and for many new teams to join the party with their own analysis attempt.
Prostate cancer (PCA) is the second most common cancer in the adult population in the UK, with over 47, 000 new cases being diagnosed each year. Over 400, 000 people assigned male at birth live with or after a diagnosis of PCA. Localised PCA is cancer that is confined in the prostate gland and has not spread to other organs. Localised PCA often grows slowly, may not give any symptoms and/or require treatment. However, occasionally this type of cancer is aggressive in nature, can spread fast and will require treatment. Patients who undergo radical treatment, such as surgery and radiotherapy, often report side effects which significantly impact their wellbeing and enjoyment of life, such as urinary and bowel incontinence, low libido, erectile dysfunction, fatigue, mood swings. Our research looks at lifestyle interventions that may help prevent PCA, as well as identifying cases when treatment may be delayed, in an attempt to best support outcomes for people with PCA.
Image by pixel2013 from Pixabay
How does treatment choice affect survival?
In the ProtecT study people were randomised to various treatments or active surveillance where no treatment is given but the patient is regularly followed-up. The study found similar chances of surviving localised PCA, with those in the active surveillance group only having a very small decrease in survival compared to the other groups. This prompted a spur of research in identifying modifiable factors which could delay PCA progression and therefore avoid unnecessary treatment.
One of the aims of our research is to look at dietary and lifestyle changes that are acceptable and achievable to PCA patients, which could reduce PCA risk and progression. These could prevent PCA or, for those who have already been diagnosed with localised disease, delay treatment and therefore avoid the associated side effects.
Dietary and physical activity interventions in people with PCA
In the PrEvENT feasibility randomised controlled trial, patients who underwent prostate removal surgery were randomly assigned to both a dietary and a physical activity intervention. The dietary intervention consisted of either:
a lycopene supplement, which is an antioxidant found in tomatoes and has been previously be suggested to be protective for PCA
eating 5 portions of fruit and vegetable per day and replacing dairy milk with a vegan option (soy, almond, oat, coconut etc)
continue as normal.
The physical activity intervention asked participants to do 30 minutes of brisk walking five times a week.
Image by PublicDomainArchive from Pixabay
For each intervention, we looked at the change in metabolites, which are very small molecules found in blood that reflect metabolic patterns, a very useful measure in diseases where there are metabolic changes, such as cancer. We found that eating more fruit and vegetables and decreasing dairy changed blood metabolite levels. Of particular interest was the change in pyruvate levels, a metabolite used as fuel in the pathway of cancer cell proliferation. This suggests that our interventions could lead to less energy being available to the proliferation of cancerous cells, which could lead to lower PCA risk and progression.
Can we predict which PCA cases do not need treatment?
A second aim of my research is to identify blood markers that can help distinguish disease that is unlikely to cause problems from aggressive disease that will advance rapidly and require treatment. We looked at the ProtecT trial and provisionally identified metabolites that could help predict PCA progression. This would allow clinicians to more accurately decide if the patient should take up treatment or if active surveillance would be appropriate.
Patients diagnosed with localised PCA have 96% chance of surviving 15 years after diagnosis. However, PCA risk factors have yet to be conclusively identified. In addition, the diagnosing techniques are invasive and there is uncertainty around which localised cases are likely to advance. More research is therefore needed to establish potential risk factors which could help prevent PCA, and blood-based markers that could predict the aggressiveness of localised PCA cases. We are also looking at the relationship between PCA risk and progression and blood DNA methylation markers, which allow cells to control the expression of genes and have previously been suggested to be responsive to both environmental factors and causes of cancer and could help us better understand the aetiology of PCA.
So what does this mean for people with prostate cancer?
Although more research is required as our studies were small and did not aim to have definitive answers, we did find some evidence to suggest that some lifestyle changes, namely increased fruit and vegetable consumption and replacing milk with non-dairy options and walking 30 minutes a day, 5 times a week are acceptable to PCA patients and that these interventions may have promising effects on blood metabolites. Identifying lifestyle factors which may have a protective role could help prevent PCA cases. Our research also identified metabolites which may help predict the aggressiveness of PCA which could help patients diagnosed with localised PCA avoid serious side effects by not undertaking unnecessary treatment.
Journal paper: Hamdy et al (2016) 10 year outcomes after monitoring, surgery, or radiotherapy for localised prostate cancer (the ProtecT trial)
Journal paper: Hackshaw-McGeagh et al (2016) Prostate cancer – evidence of exercise and nutrition trial (PrEvENT): study protocol for a randomised controlled feasibility trial.
There are an estimated 3.2 million e-cigarette users in Great Britain, and the majority of users have switched from smoking to vaping in search of a less harmful alternative to help them quit. In a recent study, people who used e-cigarettes to quit smoking were more likely to be smoke-free after one year compared to people who used more traditional methods such as nicotine patches. So, why are some smokers reluctant to try e-cigarettes, and why have some people been unable to quit smoking using them? The media, researchers, public health officials, and the general public have all played a role in discouraging some smokers from vaping.
E-cigarettes in the media
As a researcher in the field of e-cigarette use, I have often looked at news articles about vaping and felt exasperated. We frequently see e-cigarettes portrayed as a harmful option; according to many news articles, e-cigarettes are dangerous, lead to heart attacks and are as bad for your lungs as cigarettes. The same news outlets often report the opposite finding and say e-cigarettes are actually better for you. This flip-flopping leaves smokers confused and could discourage them from trying e-cigarettes for fear that vaping is actually more harmful than smoking.
Science in the media
So, why do the media keep switching their stance on e-cigarettes? They’re getting their information from the research community, and this community is divided. Some researchers claim that the costs of unknown health risks of vaping and the popularity of e-cigarettes among children and adolescents outweigh the potential benefits of helping smokers to quit, and others claim vice versa.
As researchers, we should be impartial and only provide the public with information which we can back up with evidence from our research, but, as we are still human, our opinions tend to seep through into how we report our findings and even what we choose to research. This lack of agreement in the research community is fuelling the media’s flip-flopping , leading to public confusion and reluctance to try e-cigarettes to help them quit smoking.
Public attitudes to vaping
With all of this contrasting information, it’s no wonder the general public’s opinion of vaping seems to be split too. Negative public opinion can have an impact on whether a smoker wants to try an e-cigarette. Quitting smoking isn’t easy; the last thing smokers want is to feel judged when they are trying to quit.
Negative public attitudes to vaping could put smokers off trying vaping but also affects where they can vape. Many businesses include e-cigarettes in their smoke free policies so that vapers have to stand outside with smokers. When trying to quit, it’s not ideal to be surrounded by the very thing you’re trying to wean yourself off. It’s like being on a diet and spending every meal at an all you can eat buffet when all you can eat is a salad; it’s tempting to slip into old habits. So, despite there being no indoor vaping ban (as there is with cigarettes), vapers are forced outside into a situation where they are more likely to start smoking again.
Unintended consequences of policy
It’s not just organisational policies attempting to control e-cigarette use; in 2016, a legislation called the Tobacco Products Directive (TPD) added a section on e-cigarettes in an attempt to regulate the devices. There were a number of unpopular changes to e-cigarette products as a result. Changes to the amount of nicotine allowed in products and restrictions on innovation of new products may have had unintended consequences.
With the introduction of the TPD, a limit was set on how much nicotine a vape product could contain. Nicotine is the key ingredient in cigarettes which keeps people smoking, and although it is highly addictive, nicotine is not the cigarette ingredient which is likely to kill smokers. E-cigarettes help people to quit smoking because they can contain nicotine which satisfies smokers cravings while exposing them to fewer toxins than smoking would. Limiting the amount of nicotine in these products means that heavier smokers don’t receive enough nicotine from an e-cigarette to satisfy their nicotine addiction and this makes them more likely to start smoking again.
The TPD also requires companies to register products in advance of bringing them to market. Where the e-cigarette industry was creating new, more effective devices at a very fast pace, users now can’t buy these products for a substantial amount of time after they have been developed. This restriction on innovation means that while consumers are waiting for these better products to become available, they could be trying products that don’t meet their needs. I often hear tales of “I tried one once and it was just like puffing air, so I kept smoking instead”. They have tried one product, it wasn’t good enough, and they assume all other products will be just as bad. By restricting innovation, we limit the amount of better-quality devices on the market and increase the likelihood that a smoker looking to quit will come across a poor device and turn back to smoking.
Making it easy to stop smoking
Many smokers want to quit and we, as researchers, media representatives, public health officials and even members of the public, need to make it as easy as possible for them to do so. We need to be clearer in the information we provide, be more accepting of vaping and not limit products which could help the most addicted smokers. I still have hope that smoking will be stubbed out in my generation, and that e-cigarettes could be the disruptive technology needed to help us achieve this.
Heart disease remains the leading cause of death globally, causing over 17.5 million deaths annually. Whilst death rates from heart disease are decreasing in high income countries, the most socioeconomically deprived individuals remain at the greatest risk of developing heart disease. Socioeconomic causes and the wider determinants of health (including living and working conditions, health care services, housing and a number of other wider factors) and are suggested to be the most important driver of health. Behavioural and lifestyle factors, such as smoking, alcohol consumption, diet and exercise, are the second most important contributor to health and disease.
Why does education matter?
Staying in school for longer has been shown to lead to better lifelong health, including reducing the risk of heart disease (cardiovascular disease) and dementia. We also know that those who stay in school are more likely to adopt healthy behaviours. For example, they are less likely to smoke, but more likely to eat a healthy diet and take part in physical activity. These factors, can in turn, reduce the risk of heart disease, such as by reducing body mass index (BMI) or blood pressure. We wanted to understand if these risk factors (BMI, systolic blood pressure and lifetime smoking behaviour) could explain why those who stay in school for longer are less likely to get heart disease, and how much of this effect they explained.
What did we find?
We found that individually, BMI, systolic blood pressure and smoking behaviour explained up to 18%, 27% and 34% of the effect of education on heart disease respectively. When we looked at all three risk factors together, they explain around 40% of the effect. This means that up to 40% of the effect of staying in school reducing the risk of heart disease can be explained by the fact that those who stay in school tend to lead healthier lives. In this work we looked at four outcomes, coronary heart disease (gradual build-up of fatty deposits in arteries), stroke, myocardial infarction (heart attack) and all subtypes of heart disease combined. For all the outcomes we looked at, we found similar results. Notably, the 40% combined effect is smaller than the amount estimated simply from summing the individual effects together. This suggests there is overlap between the three risk factors in how they cause heart disease.
How did we do this?
In our work, we used a few different methods and data sources to answer our questions.
We started by looking at observational data (that is the data self-reported by the participants of the study) in UK Biobank – a large population cohort study of around 500 000 individuals. Of these, almost 220 000 people were eligible to be in our analysis.
We looked at how their education affected their risk of four types of heart disease. We then looked at how the intermediate factors, BMI, blood pressure and smoking, could help explain these results.
Secondly, we replicated these analyses using two types of Mendelian randomisation analyses (a form of genetic instrumental variable analysis, see below), firstly in the UK Biobank group and secondly by using summary data from other studies in the area.
Why use genetic data?
Typically, epidemiologists collect data by asking people to report their behaviours, lifestyle characteristics and any diagnoses from a doctor. Alternatively, people in a study may have been to a clinic where their BMI or blood pressure is measured. However, this type of data can lead to inaccuracies in analyses. This could be because:
measures are not reported (or measured) accurately. For example, it can be difficult to get an accurate measure of blood pressure, where it changes throughout the day, and even just going to a clinic can result in higher blood pressure.
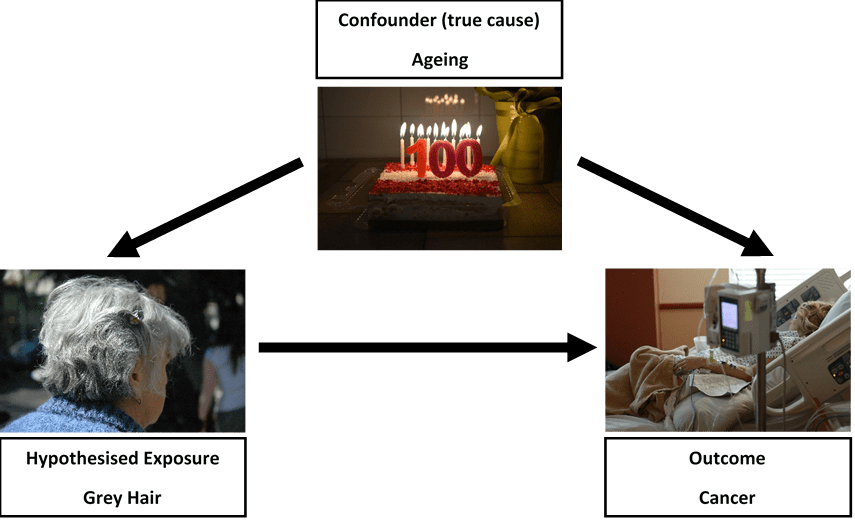
there may be other variables associated with both the exposure and outcome (confounding). One example of this is suggesting that grey hair causes cancer. Really, age is responsible for i) leading to grey hair and ii) leading to cancer. Without accounting for age, we might suggest a false association exists (see figure 1). In our study using education, this could be ethnicity for example, where it influences both staying in school and risk of heart disease.
or an individual with ill health may have been advised to change their lifestyle (reverse causality). For example, an individual with a high BMI may have had a heart attack and have been advised by their doctor to lose weight to avoid having a second heart attack.
Figure 1: Does grey hair really cause cancer?
One way to overcome these limitations is to use Mendelian randomisation. This method uses the genetic variation in an individual’s DNA to help understand causal relationships. Every individual has their own unique genetic make-up, which is determined, and fixed, at the point of conception.
We are interested in single changes to the DNA sequence, called single nucleotide polymorphisms (or SNPs). For all of our risk factors of interest (education, BMI, blood pressure and smoking) there are a number of SNPs that contribute towards the observed measures, that are not influenced by factors later in life. This means, Mendelian randomisation estimates are unlikely to be affected by bias such as confounding, reverse causality or measurement error, as we might expect when we rely on observational data. By using these genetic variants, we can improve our understanding of if, or how, a risk factor truly causes an outcome, or whether it might be spurious.
What else might be important?
Although we find BMI, blood pressure and smoking behaviour explain a very large amount of the effect, over 50% of the effect of education on heart disease is still unknown. In some small sensitivity analyses we looked at the role of diet and exercise as intermediate risk factors; however, these risk factors did not contribute anything beyond the three main risk factors we looked at. Other social factors may be involved. For example, education is linked to higher income and lower levels of workplace stress, but these factors may also be related to those we’ve looked at in this analysis.
One further suggestion for what may be responsible is medication prescribing and subsequent adherence (or compliance). For example, individuals with higher education may be more likely to be prescribed statins (cholesterol lowering drugs) compared to someone who left school earlier, but with the same requirement for medication. Subsequently, of those who are prescribed statins for example, perhaps those with higher education are more likely to take them every day, or as prescribed. We have work ongoing to see whether these factors play a role.
What does this mean for policy?
Past policies that increase the duration of compulsory education have improved health and such endeavours must continue. However, intervening directly in education is difficult to achieve without social and political reforms.
Although we did not directly look at the impact of interventions in this area, our work suggests that by intervening on these three risk factors, we could reduce the number of cases of heart disease attributable to lower levels of education. Public health policy typically aims to improve health by preventing disease across the population. However, perhaps a targeted approach is required to reduce the greatest burden of disease.
In order to achieve maximum reductions in heart disease we now need to i) identify what other intermediate factors may be involved and ii) work to understand how effective interventions could be designed to reduce levels of BMI, blood pressure and smoking in those who leave school earlier. Additionally, our work looked at predominantly European populations, therefore replicating analyses on diverse populations will be important to fully understand the population impact.
We hope this work provides a starting point for considering how we could reduce the burden of heart disease in those most at risk, and work to reduce health inequalities.
Depression is one of the biggest public health challenges we’re currently facing and is expected to be the highest global burden of disease by 2030. The world health organisation (WHO) estimates that around 300 million people worldwide currently experience depression and that at least one in five people will experience depression at some stage of their life. Treatment is not always successful with only around 40-60% of individuals responding positively to antidepressant medication, and other forms of treatment such as cognitive behavioural therapy (CBT) or other talking based therapies requiring long waiting times of up to two years. It’s no surprise to see that depression and other mental health treatments are considered to be in a ‘crisis’ as we continually look for new and effective ways to combat this disease.
Research suggests that depression may first begin to manifest early in adolescence and young adulthood. This may have serious downstream consequences as depression during adolescence is related to both concurrent and later self-harm and suicide, corresponding mental health problems (like anxiety, addiction and psychosis) and impaired social functioning (reduced cognitive functioning and reclusiveness), to name a few. It also appears that depression during adolescence and young adulthood may actually be getting worse. Now whether or not this is because young people are talking more about their mental health than before remains to be seen, but that has not stopped researchers identifying potential causes for depression in adolescence in the hope of developing new and effective treatments and interventions. The message seems to be clear: by stopping/reducing depression in young people, we can potentially improve the quality of life later on.
What is responsible for depression in young people?
The lived experience of depression between young people differs from one person to the next, meaning there is no ‘one-size-fits-all’ approach. But with the help of research, we have begun to identify things that individuals experiencing depression have in common, that could be useful for treating and even preventing depression in young people. What follows is a whistle stop tour of some of the findings of potential causes of depression in young people.
Bullying
It may seem obvious, but childhood and adolescent bullying is one of the strongest predictors of current and later depression. One recent study found that individuals who had been bullied during adolescence were almost 3 times more likely to be depressed at age of 18. Bullying is particular prevalent during school years but can also occur well into the workplace or later education, which can have lasting effects on an individual’s mental health. Stopping bullying from occurring will be difficult, but that does not mean we cannot support individuals who have been bullied in order to help prevent depression from occurring or getting more severe.
Parental Depression
A lot of research has focused on the role of parental mood and later depression in young people. The role of parenting cannot be understated as numerous studies have shown that children of depressed parents are more likely to go on to have depression themselves, see research by Pearson et al,Stein et al and Gutierrez-Galve et al. However, it’s not clear if this is passed on genetically from the parent to child, or if there is something in the “environment” that transmits depression from parent to child. Whilst we don’t know for sure, the answer looks like it could be a bit of both. Parents may pass on depression genetically to their children, but depressed parents may also create an environment that makes the child more liable to depression. It is even possible that the parent passes on their genetics and the child then creates an environment for themselves that makes them more liable to depression. This is a form of gene-environment correlation that I won’t discuss in detail, but research is beginning to tease this apart with regard to parent and childhood depression.
Genetics
Interest in the genetics of depression has been heightened in the last few years. We always knew from twin studies that depression was likely to be heritable (i.e., that depression can be passed on from generation to generation), but convincing some that depression could have a strong genetic basis was tough (for a really good debate on this involving Professor Marcus Munafò, you can listen to this episode of BBC Start the Week). Most recently it has been shown that common genetic variants associated with depression in adulthood seem to predict greater levels of depression in children and adolescents, as well as varying patterns of depressive mood across adolescence. Importantly, it’s clear that there is no ‘one gene’ for depression. Instead, there are multiple genes which can be referred to as ‘polygenicity’ or ‘polygenic risk scores’; “poly” meaning multiple and “risk” indicating that individuals carrying multiple risk genes are more liable or ‘at risk’ to depression. By using polygenic risk scores we can begin to identify individuals experiencing depression early by using knowledge of their genetic make-up. However, it is really important to state here that genetic liability to depression does not equal genetic determinism. Just because someone is more genetically liable to depression, does not mean they will get depressed. There are multiple other factors at play, and we do not know how genetic liability to depression impacts on other pathways (i.e., does having genetic liability make you more likely to seek out an environment that could leave you more depressed?); but many researchers are beginning to ask these questions.
Taken together, these findings highlight how diverse depression is and how many factors could underlie depression in adolescence. There are a ton of other factors that have been related to adolescent depression that I have not had time/space to talk about. That is not to say they are not important, because most likely some are. As research develops and we are able to utilise different methods, we will get a better picture of what underpins depression in adolescence and what can be done to prevent and treat it.
What can we do?
Well for one, we have to keep up the research. We don’t know nearly enough about the underlying mechanisms and pathways that truly underlie adolescent depression. Researchers are beginning to examine this further with novel and promising techniques, but we also have to streamline the time it takes for research to be put into practise. The prolific mental health blog “The Mental Elf” states that it takes 17 years for research to reach clinical practise. That’s a long time and means a lot of people could miss out on the treatment they deserve.
Secondly, we have to be more forthright in how we talk about depression. You may have heard the expression ‘it is ok to be not be ok”. Avoiding telling people to “man-up” when they’re feeling depressed, speaking out and campaigns will only drive this forward. We have to normalise the fact that depression is a disease and like any other disease, it is good to talk about it. Only by talking about depression can we really move forward to end the stigma that being depressed is some kind of weakness. In fact one of my favourite instances of this recently was well explained by the England international Danny Rose.
Where do we go from here?
We appear to be reaching a turning point where more and more people are discussing mental health issues. This may be celebrities, royals or just your average Jo from down the street. But what is important is that we recognise the problem. That depression is a global burden that may be getting worse and requires our utmost attention and action. We are beginning to understand the causes of depression and how we might tackle it through research and reducing the social stigma that surrounds depression. However, the question is whether or not we can take advantage of these changes to really make a difference. Can we build on the progress we have made to finally one day beat depression? Yes. I really believe we can.
There are some awesome twitter feeds out there who I have always found to be really helpful and supportive of mental health issues. These people really get depression and are leading the charge in one way or another so do please give them a follow:
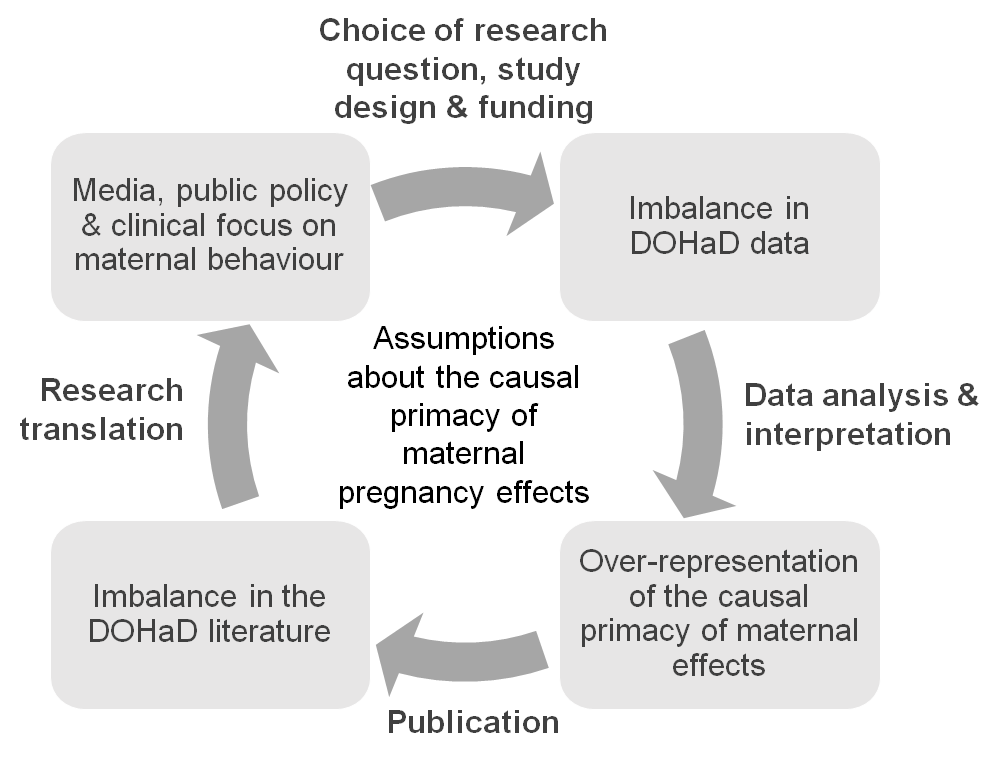
For many years, researchers have been studying how our early life experiences, including those that happen before we are born, can affect our lifelong health. In an article we wrote last year, Debbie Lawlor (University of Bristol), Sarah Richardson (Harvard University) and I show that most of these studies have focused on the characteristics and behaviours of mothers around the time of pregnancy. In a recent paper published in the Journal of Developmental Origins of Health and Disease, Debbie Lawlor, Sarah Richardson, Laura Schellhas and I show that there have been more studies of maternal prenatal influences on offspring health than any other factors (read more here).
We argue this is because people assume that mothers, through their connection to the developing fetus in the womb, are the single most important factor in shaping a child’s health. This assumption runs deep and is reinforced at every level, from researchers, to research funders, to journalists, to policy makers, to health care professionals and the general public (see figure 1).
In our article, we question the truth behind this assumption.
Is there a strong scientific rationale for studying pregnant mothers so intensively?
Well, no actually. Although a lot of studies have found correlations between maternal characteristics and offspring health, the evidence that these characteristics actually have a causal effect is pretty weak. And since there haven’t been many studies of the effects of fathers and other factors, it’s difficult to say how important any maternal effect might be compared to any other early life experience.
Focusing so intensively on pregnant mothers, and interpreting all evidence as causal (if a mother does X, their unborn child will have Y), can have very damaging effects. Complex, nuanced scientific findings are being rushed into simplified advice that, although well-meaning, places the burden of blame on individual pregnant women. For example, there has been very little research on the effects of low-level drinking during pregnancy, but the current advice in the United States is for all sexually active women of reproductive age to avoid alcohol completely if they are not using birth control, for fear of fetal harm.
Fig. 1 Assumptions that the health, lifestyle and behaviours of mothers around the time of pregnancy have the largest causal influence on their children’s health and risk of disease drives research at all stages, from study design to research translation, and is also reinforced by research itself.
A culture of blame
The culture of blame is more overt in the media, where articles are often guilty of scaremongering. This feeds into public beliefs about how pregnant women should and shouldn’t behave, which can limit pregnant women’s freedom and even lead to questions around whether their behaviour is criminal. For example, pregnant women have reportedly been refused alcoholic drinks in bars, and taking drugs during pregnancy is legally classed as child abuse in many US states.
In our article, we make a number of recommendations that we hope will create more of a balance. In particular, we call for more research on how child health might be influenced by fathers and other factors, including the social conditions and inequalities that influence health behaviours. We also call for greater attention to be paid to how health advice to pregnant women is constructed and conveyed, with clear communication of the supporting scientific evidence to allow individuals to form their own opinions.
The EPoCH study
In June, I’ll begin work on a new project to investigate how both mothers and fathers’ lifestyles might causally affect the health of their children. Funded by the Medical Research Council, the EPoCH (Exploring Prenatal influences on Childhood Health) study will highlight whether attempts to improve child health are best targeted at mothers, fathers or both parents. I’m excited to work closely with the people behind WRISK to help ensure that findings from this project are communicated effectively and responsibly.
I hope that, along with the rest of the research community, we can produce high quality evidence to support health care and advice that maximises the health of all family members and stops blaming women for the ill health of the next generation.
The original article can be accessed (open access) here, and the authors’ full list of recommendations can be found below.
Full recommendations
Our full recommendations, which apply variously to researchers, journalists, policy makers and clinicians:
Collect more and better quality data on partners of pregnant women.
In addition to studying the effects of mothers, study and compare the effects of partners/fathers, social and other factors on child health.
Look for causal relationships between these factors and child health, not just (potentially spurious) correlations.
Publish all results, including negative results, to give a balanced view of the evidence.
Be aware and critical of the current imbalance in the scientific literature and how this will bias our overall understanding of the truth.
Collaborate with social scientists to consider the social implications of this research and the role of cognitive bias and social assumptions when interpreting findings.
When communicating findings, put the risk in context: compare findings to the broader scientific literature and the social environment.
Avoid language that suggests individual mothers are responsible for direct harm to their foetuses (most of the evidence will be based on averages in a population and can’t be assumed to apply to all individuals).
Where there is evidence of a paternal effect, aim public health advice at both parents.
Explain the level of risk in a way that empowers people to assess the evidence and form their own opinions (i.e. avoid over simplification).
This blog post is an edited version of one originally posted on the WRISK project website.
 Kayleigh Easey, a PhD student and member of the Tobacco and Alcohol Research Group (TARG) at the School of Psychological Science at the University of Bristol, takes a look at a recent systematic review investigating effects of parental alcohol use and offspring mental health.
Kayleigh Easey, a PhD student and member of the Tobacco and Alcohol Research Group (TARG) at the School of Psychological Science at the University of Bristol, takes a look at a recent systematic review investigating effects of parental alcohol use and offspring mental health.